


TRANSFORMING PUBLIC HEALTH IN INDIA: A REVIEW OF TECHNOLOGICAL INNOVATIONS ACROSS NATIONAL HEALTH PROGRAMS
HTML Full TextTRANSFORMING PUBLIC HEALTH IN INDIA: A REVIEW OF TECHNOLOGICAL INNOVATIONS ACROSS NATIONAL HEALTH PROGRAMS
Imran Ali Dar, Satpal Kushwaha *, Tanya Sharma and Ranjan Kr. Singh
Faculty of Pharmaceutical Sciences, Mewar University, Gangrar, Chittorgarh, Rajasthan, India.
ABSTRACT: The National AIDS Control Programme (NACP) has been a cornerstone of India's comprehensive, technology-driven strategy to address non-communicable diseases, maternal health, and mental health since the country's independence. Phase V of NACP (2021–2026) seeks to eradicate HIV/AIDS as a public health threat by 2030 through a rights-based, inclusive approach, and this overview looks at how the NACP has changed and what impact it has had on the country's public health. The paper addresses the pathogenesis, transmission, and treatment of HIV, highlighting India's considerable epidemiological successes: a 49% reduction in new infections and an 80% fall in AIDS-related deaths between 2010 and 2026. Key to these breakthroughs is the merging of modern medical and digital advancements, including: Medical Breakthroughs: The creation of low-cost, generic versions of long-acting injectables like Lecavalier for pre-exposure prophylaxis (Prep). Digital Transformation: The implementation of the Strategic Information Management System (SIMS) for real-time tracking and the spread of telemedicine for antiretroviral medication (ART) delivery.
Keywords: National AIDS Control Programme (NACP), National AIDS Control Organisation (NACO), NACP Phase V (2021-2026) and Ayushman Bharat. Ministry of Health and Family Welfare (MOHFW), National Health Policy (NHP), Medical & Treatment Terminology, Antiretroviral Therapy (ART) Ministry of Health and Family Welfare (MOHFW), National Health Policy (NHP), Medical & Treatment Terminology etc
INTRODUCTION: A technology-driven, patient-centric ecosystem is replacing old, facility-centric models in India's healthcare system, which is now going through a dramatic transition. The incorporation of cutting-edge technical advancements like eSight and AI-driven treatments into the nation's National Health Programs is at the centre of this transition. These innovations, which are driven by the Ayushman Bharat Digital Mission's (ABDM) goal, are evolving from luxury treatments to crucial elements of public health service. A major advancement for the National Programme for Control of Blindness and Visual Impairment (NPCBVI) is a breakthrough in electronic vision enhancing technology.
eSight overcomes the limits of conventional optical aids by projecting real-time pictures onto high-resolution displays for the visually impaired using high-speed cameras and sophisticated algorithms. Its incorporation into treatment plans demonstrates India's dedication to "Digital Inclusion," guaranteeing that people with impaired vision may benefit from technology and become more socioeconomically independent 1.
An innovation in electronic vision-enhancing technology is a significant development for the National Programme for Control of Blindness and Visual Impairment (NPCBVI). By projecting real-time images onto high-resolution screens for the visually handicapped utilising highspeed cameras and complex algorithms, eSight surpasses the limitations of traditional optical aids. India's commitment to "Digital Inclusion," which ensures that those with vision impairments may benefit from technology and become more socioeconomically independent, is demonstrated by its integration into treatment regimens. These developments signify a strategic shift in the direction of precision and preventative medicine. India is establishing a worldwide standard for scalable, tech-enabled public healthcare by combining state-of-the-art equipment like the strong framework of National Health Programs 2.
Enhancing the Health System: Building a robust, egalitarian, and effective network that can provide all residents with high-quality care especially during public health emergencies is the key to strengthening a health system. This calls for a multifaceted strategy that goes beyond simply constructing hospitals in the context of healthcare modernization, as the present attempts in India.
Improving Primary Treatment Infrastructure: Putting more emphasis on proactive, community-based treatment rather than reactive hospital care. At the local level, programs like the creation of Health and Wellness Centre’s seek to offer complete primary healthcare, prenatal services, and chronic illness screening.
Encouraging the Health Workforce: The strength of a system depends on its personnel. In addition to hiring more physicians and nurses, this entails up skilling frontline community health workers (such as ASHA employees) and incorporating them into the digital ecosystem. Expanding centralized health data systems (like the Ayushman Bharat Digital Mission) to provide interoperable medical records is one way to advance digital health information. This enhances continuity of care, enables telemedicine, and allows governments to track health trends and allocate resources efficiently 3.
Financial Risk Protection: Putting in place comprehensive health insurance programs to provide "Universal Health Coverage." The objective is to significantly lower disadvantaged people' catastrophic out-of-pocket costs when they suffer from serious diseases. Strengthening Supply Chains ensuring that sophisticated diagnostics, cutting-edge therapies, and necessary medications are distributed consistently and fairly to both urban and rural areas.
HIV/AIDS: Acquired immunodeficiency syndrome (AIDS) and the human immunodeficiency virus (HIV) are two of the most important public health issues in modern medicine. Although the phrases are frequently used synonymously, they relate to different phases of the same illness.
HIV (Human Immunodeficiency Virus: The infection is brought on by this virus. HIV targets CD4 cells, also known as T cells, which aid the body's defenses against infections. HIV lowers the body's CD4 cell count if treatment is not received, leaving the patient more susceptible to infection-related malignancies or other infections.
AIDS (Acquired Immunodeficiency Syndrome): This is the most serious and advanced stage of HIV infection. When an individual's immune system is seriously compromised, their CD4 cell count falls below a certain threshold, or they contract particular opportunistic illnesses, they are diagnosed with AIDS.
The Modern Reality: A Manageable Condition: HIV was a deadly diagnosis when it was first discovered in the 1980s since an infection nearly always led to AIDS. The terrain has drastically changed since then.
Antiretroviral Therapy (ART): HIV is currently a chronic illness that is very treatable. ART lowers the viral load (amount of virus in the blood) to an undetectable level when used as directed. In addition to protecting the immune system and preventing HIV from progressing to AIDS, this also stops the virus from spreading sexually to other people, a concept known as U=U (Undetectable = Untransmutable). In order to ensure that individuals living with HIV can live long, healthy, and meaningful lives, the current worldwide focus in the fight against HIV/AIDS is on comprehensive sex education, broad access to routine testing, early treatment start, and the elimination of societal stigma 4.
Signs and Symptoms Differ Depending on Stage: Depending on the stage of the infection, HIV manifests itself in a variety of ways. If treatment is not received, the illness advances through three primary phases, each of which has distinct clinical symptoms.
Stage 1: Acute HIV Infection: Many (but not all) persons get a severe flu-like sickness two to four weeks after the virus enters the body. As the virus replicates quickly, this is the body's first immunological reaction. Common Symptoms: Fever, chills, exhaustion, sweats at night, pains in the muscles, sore throat, enlarged lymph nodes (especially in the neck), rash, and mouth ulcers are common symptoms.
People frequently be unaware that they have HIV since these symptoms are so similar to those of common viral infections like the flu or mononucleosis. During this phase, some people might not have any symptoms at all.
Stage 2: Clinical Latency (Chronic HIV Infection): The virus enters a phase of clinical latency after the acute stage. The virus is still alive and growing throughout this period, but very slowly. Common Symptoms: Most people either have extremely minor symptoms or are asymptomatic, meaning they have no symptoms at all. Progression: Although some people may advance more quickly, this phase can continue ten years or more without medicine. The virus can still spread to other people at this stage. However, a person can stay in this stage for the rest of their life and maintain an undetectable virus load provided they take daily Antiretroviral Therapy (ART) as directed. (Preventing transmission).
Stage 3: Acquired Immunodeficiency Syndrome (AIDS): When the immune system has been seriously compromised, the illness reaches its most advanced stage. In this stage, opportunistic infections or malignancies that prey on the compromised immune system are more likely to produce symptoms than the HIV virus itself.
Pathophysiology: HIV infects and kills CD4+ T cells, which are critical for the immune response. Its life cycle includes of binding, fusion, reverse transcription, integration into host DNA, replication, assembly, and budding/maturation.
The absence of CD4+ T cells exposes the body to opportunistic infections. Antibodies, antigens, or the virus itself can be detected in blood or saliva using tests such as ELISA, Western Blot, or PCR. There is a temporal interval between exposure and quantifiable infection. AIDS is diagnosed when CD4 counts fall below 200 cells/mm³ or opportunistic infections arise 5.
Prevention: A comprehensive strategy that incorporates safe habits, medical treatments, and routine testing is needed to prevent HIV/AIDS. Since certain physiological fluids blood, semen, vaginal fluids, rectal fluids, and breast milk are the means by which HIV is spread, preventative techniques concentrate on preventing these pathways.
Biomedical Interventions (Medication-Based):
(Pre-Exposure Prophylaxis: Those who do not already have HIV but are at a high risk of contracting it take this daily tablet (or long-acting injectable). It is quite efficient in preventing HIV from sex and injection drug use when taken as directed.
PEP (Post-Exposure Prophylaxis): This is an emergency drug administered following a possible HIV exposure (e.g., unprotected intercourse with an HIV-positive partner, condom rupture, or needle stick injury). For PEP to be effective, it must be initiated within 72 hours after the exposure.
Treatment as Prevention & U=U: An individual with HIV cannot sexually spread the virus to their partners if they take antiretroviral therapy (ART) on a regular basis and reach an undetectable viral load. This idea is sometimes referred to as U=U (Undetectable = Untransmutable).
Behavioral and Barrier Methods: The danger of transmission is greatly decreased by the proper and consistent use of physical barriers and protective practices.
Condom Use: One of the best methods to avoid HIV and other sexually transmitted infections (STIs) is to always use male or female condoms appropriately during vaginal, anal, or oral sex.
Safe Injection Practices: It is essential for drug injectors to never share syringes, needles, or other injection supplies. The possibility of blood-borne transmission is eliminated by always using brand-new, sterile equipment.
Public Health and Medical Procedures: At the population level, routine medical procedures are crucial in stopping the spread of HIV. Prevention of Mother-to-Child Transmission (PMTCT): During pregnancy, delivery, or nursing, HIV-positive pregnant women might infect their unborn children. However, the risk of transmission is reduced to less than 1% if the mother is detected early, takes ART during her pregnancy, and gives HIV medication to the newborn.
Regular Testing and Screening: The first step in preventive is understanding one's condition. Frequent screening enables early discovery, prompt treatment, and the stop of further transmission.
Blood Safety Procedures: Since all donated blood, organs, and tissues are thoroughly tested for HIV and other blood-borne infections in contemporary medical systems, transfusion related transmission is incredibly uncommon. By combining these strategies using protection, utilizing preventive medications like Prep, and ensuring regular testing the transmission of HIV can be effectively halted 6.
Diet and Nutrition: Nutrition and a healthy diet are essential to HIV management. A balanced diet and antiretroviral therapy (ART) work together to boost immunity, maintain a healthy weight, and improve the body's ability to absorb drugs, even if food cannot cure the virus.
Macronutrients: People with HIV frequently need more energy (calories) and structural support (protein) than people without the infection because their bodies are working harder to combat the virus. High-quality protein is necessary for maintaining muscle mass and developing a robust immune system. Lean meats, poultry, fish, eggs, dairy, beans, lentils, and nuts are all excellent sources.
Complex Carbohydrates: The body uses carbohydrates as its primary energy source. Eat a lot of whole, unprocessed foods, such as sweet potatoes, brown rice, oats, whole-wheat bread, and a range of fruits and vegetables. Additionally, they offer vital fiber, which aids in controlling insulin resistance a possible adverse consequence of many HIV drugs.
Healthy Fats: Fats aid in the body's absorption of vital vitamins and offer additional, substantial energy. Limit saturated and trans fats and choose unsaturated fats from foods like avocados, almonds, seeds, olive oil, and fatty seafood like salmon 7.
Hygiene: For someone with a weakened immune system, this is one of the most important parts of diet. A person with advanced HIV may experience severe or perhaps fatal foodborne diseases that would only cause little pain in a healthy individual. Cook Completely Make sure all fish, poultry, and meats are cooked to safe internal temperatures. Steer clear of undercooked or raw eggs (as in homemade mayonnaise).
Avoid High-Risk Foods: Steer away of raw sprouts, unpasteurized milk or cheeses, and raw seafood (sushi, oysters). Wash Carefully: Before consuming any fresh produce, give it a thorough wash in clean water. Use different chopping boards and knives for fresh produce and raw meats to avoid cross-contamination.
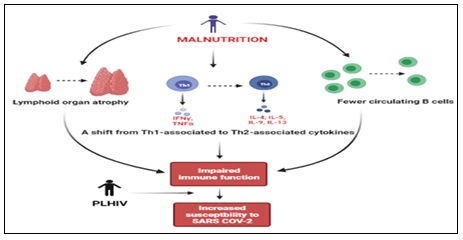
FIG. 1: MALNUTRITION CYCLE
Strict Food Safety and
For Nausea: Eat small, frequent meals rather than three large ones. Stick to bland, low-fat foods like crackers, plain rice, or toast. Ginger tea can also help settle the stomach. For Diarrhea: Stay heavily hydrated to replace lost fluids. Follow the BRAT diet (Bananas, Rice, Applesauce, Toast) and avoid greasy, fried, or highly spiced foods, as well as dairy, which can irritate the gut. For Loss of Appetite: Focus on nutrient-dense foods. If eating solid food is difficult, high calorie, high-protein smoothies or nutritional shakes can be an effective alternative.
Hydration and Micronutrients:
Water: Consume eight to ten glasses of safe, pure water each day. Water keeps the body from being dehydrated, helps transport nutrients throughout the body, and eliminates the metabolized byproducts of drugs. Vitamins and Minerals: Although the majority of essential micronutrients should be found in a balanced diet, individuals with HIV may have decreased levels of zinc, selenium, vitamin A, vitamin B vitamins, vitamin C, and vitamin E. A typical daily multivitamin may be advised by a healthcare professional; however, "mega-dosing" supplements should be avoided as they may conflict with HIV drugs 8.
Epidemiology: The study of how a disease spreads among communities and the variables that affect or define its distribution is known as epidemiology. Public health professionals can better understand who is contracting HIV/AIDS, where they reside, how the virus spreads, and if interventions are effective by using epidemiological data.
The Global Burden (Prevalence and Incidence): Despite tremendous progress in containing the pandemic, HIV is still a significant worldwide public health concern. Based on current UNAIDS data:
Prevalence (People living with HIV): Approximately 39 million people globally are living with HIV.
(New Infections): Every year, there are around 1.3 million new cases of HIV infection. Since its high in the mid-1990s, this figure has been gradually decreasing, mostly as a result of preventative initiatives and treatment as prevention (U=U).
Mortality: AIDS-related diseases claim the lives of over 630,000 individuals annually. This sharp decline from the mid-2000s high is clearly related to the widespread use of antiretroviral therapy (ART) 9.
Geographic Distribution: HIV is not uniformly dispersed throughout the world; rather, it is concentrated in some areas.
Sub-Saharan Africa: Approximately two-thirds (more than 25 million) of all HIV-positive individuals worldwide reside in this region, which is the epicenter of the pandemic. Women and girls make up a disproportionate share of new infections in this area.
Asia and the Pacific: The second-highest number of HIV-positive individuals reside in this area. With over 2.4 million HIV-positive individuals, India has the third-largest HIV pandemic worldwide. However, the overall adult incidence rate is really quite low (around 0.2%) due to India's large population.
Geographically, the disease is centered in India; traditionally, it has been more common in southern states like Andhra Pradesh and Karnataka and northeastern areas like Mizoram and Nagaland, which are mostly affected by injectable drug usage 10.
Demographics and Populations: Epidemiologists monitor "key populations" groups of individuals who have a markedly increased risk of contracting HIV because of biological, social, or legal circumstances. The risk of contracting HIV is much increased worldwide for:
Individuals who Inject Drugs (PWID): The virus enters the bloodstream immediately when infected needles are shared.
Men who have Sex with Men (MSM): Compared to vaginal sex, receptive anal sex presents a greater biological risk of transmission.
Sex Workers and their Clients: Because condom use varies and they have several sexual partners. People who identify as transgender frequently experience extreme stigma, discrimination, and difficulties getting access to healthcare.
Principal Transmission Modes:
Heterosexual Contact: Heterosexual intercourse is the primary source of HIV infections globally, particularly in Sub-Saharan Africa.
Male-to-Male Sexual Contact: This is still the major way that new illnesses are spread in many Western countries and regions of Latin America.
Blood-Borne Transmission: Mostly via common injecting equipment. In nations with advanced medical screening, transfusions are now quite uncommon.
Mother-to-child: Transmission that occurs during pregnancy, delivery, or nursing is known as vertical transmission. The efficacy of screening and treating HIV-positive pregnant women has caused this route to decline worldwide.
The "95-95-95" Targets: Epidemiologists and international health organization’s use the UNAIDS "95-95-95" cascade of care objectives to monitor the epidemic's progress, 95% of HIV-positive individuals are aware of their status. 95% of individuals with a diagnosis are on long-term ART.
Viral suppression (undetectable viral load) is attained by 95% of ART patients. By monitoring these measures, nations may pinpoint areas where their healthcare systems fall short, whether it be in testing, drug adherence, or connection to treatment 11.
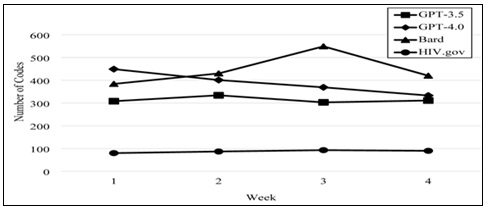
FIG. 2: MONITORING THESE MEASURES, NATIONS MAY PINPOINT AREAS WHERE THEIR HEALTHCARE SYSTEMS FALL SHORT, WHETHER IT BE IN TESTING, DRUG ADHERENCE, OR CONNECTION TO TREATMENT
(NACP) Genesis and Evolution: India's NACP (NACP I) was launched in 1992 with World Bank assistance with the aim of reducing transmission. Later phases (NACP II, III, and IV) used decentralised strategies, extended interventions, improved preventative measures, and integrated services. The government completely funds the NACP Phase V (2021–2026), which has a budget of ₹15471.94 crore. In line with UN Sustainable Development Goal 3.3, it aims to eradicate the HIV/AIDS epidemic as a public health threat by 2030. It focuses on comprehensive prevention, detection, and treatment, equity and inclusion for high-risk and vulnerable populations, and a decrease in stigma and discrimination.
Successes and Challenges: International recognition has been given to NACP for boosting access to ART and lowering new HIV infections by 48% (compared to a global average of 31%). Obstacles include enduring stigma and discrimination, gaining access to important populations, managing finances and human resources, managing co-infections (TB, hepatitis), and eradicating mother-to-child transmission. In order to assess the effectiveness of public health programs, it is necessary to consider both the past successes and the current challenges. A complicated picture of enormous logistical victories combined with enduring social and structural difficulties emerges when examining India's larger National Health Programs in addition to the particular battle against HIV/AIDS 12.
National Health Programmes (India): Some of the biggest public health initiatives in the world are run by India. These programs have evolved over the last several decades from discrete disease-control initiatives to all-encompassing, system-wide frameworks such as Ayushman Bharat.
Historic Eradications: The complete eradication of maternal and neonatal tetanus and polio (certified in 2014) is proof of the effectiveness of India's grassroots health workers and immunisation campaigns.
Maternal and Child Health: The Maternal Mortality Ratio (MMR) and Infant Mortality Rate (IMR) have significantly decreased as a result of initiatives like the Janani Suraksha Yojana (JSY), which have effectively encouraged institutional deliveries.
Financial Risk Protection: The implementation of PM-JAY (Pradhan Mantri Jan Arogya Yojana) has reduced catastrophic out-of-pocket medical costs and given millions of low-income household’s accesses to health insurance.
Digital Leapfrogging: Even in rural locations, the quick uptake of telemedicine (Sanjivani) and the drive for digital health records (Ayushman Bharat Digital Mission) are effectively democratising access to professional consultations.
The Challenges:
The Rural-metropolitan Divide: In contrast to metropolitan areas, rural and tribal areas continue to have a serious lack of specialised physicians, state-of-the-art diagnostics, and properly equipped institutions.
The Double Burden of Disease: India's healthcare system is overburdened with treating both non-communicable illnesses (NCDs) including diabetes, cancer, and cardiovascular disease as well as conventional communicable diseases like malaria and tuberculosis.
Healthcare Financing: Although it has improved, India's public health spending as a proportion of GDP still falls short of worldwide standards, placing strain on public facilities and frequently driving patients into pricey private treatment.
Reversing the Pandemic: The HIV pandemic was effectively stopped and reversed in India.
Since the epidemic's peak, both new infections and AIDS-related fatalities have drastically decreased by more than 80%.

FIG. 3: MAIN THEME: DISCLOSURE SUCCESS AND CHALLENGES
Free Antiretroviral Therapy (ART): Achieving the U=U benchmark and saving lives have been made possible by the government’s dedication to offering free, lifetime ART to anybody who tests positive for HIV.
Targeted Interventions: Long before it was socially acceptable to do so, the NACP was successful in working with NGOs and community-based organisations to directly provide safe sex education, condoms, and clean needles to "high-risk" populations (sex workers, men who have sex with men, and injecting drug users) 13.
Prevention of Mother-to-Child Transmission: The number of infants born with HIV has significantly decreased because to routine screening of expectant mothers and prompt medical management.
Persistent Discrimination and Stigma: This continues to be the greatest obstacle. Many people avoid being tested or picking up their prescription from public clinics out of fear of social rejection.
Late Presenters: Due to the stigma noted earlier, a sizable portion of individuals are still only identified when their immune systems are already seriously weakened (Stage 3/AIDS), which makes treatment considerably more challenging.
Reaching Marginalised Groups: Despite the existence of specific treatments, it is still challenging to reach the most marginalised groups, such as transgender persons or drug injectors, because of overlapping social, legal, and financial hurdles.
Financing Fatigue: The viability of free ART programs may be threatened by domestic and international financing stalling as HIV is increasingly seen as a treatable chronic illness rather than an acute catastrophe. Both general health programs and the HIV response demonstrate that, although government regulations and medical technology can offer the means for success, community involvement and the removal of social stigmas are necessary to complete the task 14.
Vision: Continuing efforts in prevention, testing, treatment, and care, as well as a strong commitment to lowering stigma and prejudice while preserving equitable access.
Achieving ambitious goals requires community involvement and integration with larger healthcare systems. India's goal is in line with UNAIDS's global objective of eradicating AIDS as a public health concern by 2030, which is summed up as "zero new infections, zero discrimination, and zero AIDS-related deaths." The National AIDS Control Programme (NACP), which is presently in its fifth phase (NACP-V, 2021-2026) and is managed by the National AIDS Control Organization (NACO) under the Ministry of Health, accomplishes this purpose 15.
Major Breakthroughs: Recent national evaluations indicate that India has done exceptionally well. The number of new HIV infections decreased by more than 49% between 2010 and 2026. Nearly that time, the number of AIDS-related deaths fell by nearly 80%. The transmission from mother to kid has decreased by almost 75%, suggesting that early identification and treatment should start during pregnancy. While treatment coverage increased from 1.49 million to 1.86 million HIV positive individuals, testing coverage increased from 41 million (2020–21) to 66 million (2024– 26) 16.
Long-acting HIV Prevention shots Lenacapavir: Lenacapavir is a six-month injectable (pre-exposure prophylaxis) that has been demonstrated to offer almost total protection against HIV transmission. India is anticipated to take the lead globally in developing inexpensive, generic versions of this medication. Approved generics from Indian producers (Dr. Reddy's, Hetero, Emcure, and Mylan) will make this innovation accessible in 115 low- and middle-income countries when India has finished regulatory licensing 17.
The Digital Health and Data System: By tracking testing, treatment, and results in real time, Naco’s Strategic Information Management System (SIMS) improves planning and transparency. Antiretroviral treatment (ART) is more accessible because to telemedicine and consultations, particularly in rural and impoverished areas 18.
Integration of AI and Diagnostics: While point-of-care molecular testing enables quick identification and treatment, AI powered diagnostics assist in identifying early infection patterns 19. India's achievement shows how community involvement, scientific creativity, and political resolve can all come together to change the trajectory of an epidemic 21. Right now, the country is concentrating on: Reaching the 95-95-95 targets (95% of HIV positive individuals are aware of their status, 95% are receiving treatment, and 95% have attained viral suppression).
Long-acting preventative medications are being introduced more often to maintain momentum in the improvement of stigma-free and inclusive healthcare systems 20. India's past demonstrates that HIV/AIDS may be eliminated as a public health emergency by 2030 with continued innovation and equitable access 21, 22.
CONCLUSION: In conclusion, one of the most important public health accomplishments in India's history is the National AIDS Control Programme (NACP), which was implemented in response to HIV/AIDS. From its first years of crisis management to the present Phase V (2021–2026), the program has developed into an all-encompassing, technology-driven, rights-based framework that combines prevention, treatment, and care with more general efforts to reform the health system. The impressive drop in new infections and AIDS-related fatalities highlights the value of evidence-based interventions, community involvement, and persistent governmental commitment. Combining biological technologies like antiretroviral treatment (ART), pre-exposure prophylaxis, and new long-acting injectables with technology innovations like telemedicine and real-time data systems is a major strength of India's strategy.
In addition to increasing access and adherence, these developments have turned HIV from a deadly illness into a chronic condition that can be controlled. Furthermore, a more accessible and inclusive healthcare ecosystem has been made possible by alignment with national efforts like Ayushman Bharat and the Ayushman Bharat Digital Mission. But there are obstacles in the way of eradicating HIV/AIDS as a danger to public health by 2030. Progress is nonetheless hampered by persistent stigma, delayed diagnosis, unequal access for marginalised groups, and budget limitations. In addition to consistent institutional and financial support, addressing these obstacles would need increased community awareness, policy backing, and focused outreach. In the end, India's experience shows that combating HIV/AIDS necessitates a comprehensive strategy that incorporates social justice, technical advancement, and public health governance. India is well-positioned to realise the goal of "zero new infections, zero discrimination, and zero AIDS-related deaths," setting a worldwide standard for HIV/AIDS eradication, if present momentum is sustained and any gaps are successfully filled.
ACKNOWLEDGEMENT: Nil
CONFLICT OF INTEREST: Nil
REFERENCES:
- Pradeep Kumar D of SIM (Surveillance and E. Editorial Commentary. 2022; Available from: http://naco.gov.in/elimination-
- Baeten JM, Palanee-Phillips T, Mgodi NM, Mayo AJ, Szydlo DW and Ramjee G: Safety, uptake, and use of a dapivirine vaginal ring for HIV-1 prevention in African women (HOPE): an open-label, extension study. Lancet HIV 2021; 8(2): 87–95.
- Beegle S, Gomez LA, Blackard JT, Yan B, Robertson J and Fedders KT: HIV Prevention and Treatment Information from Four Artificial Intelligence Platforms: A Thematic Analysis. AIDS Behav 2025; 29(11): 3394–403.
- Bertman V, Petracca F, Makunike-Chikwinya B, Jonga A, Dupwa B and Jenami N: Health worker text messaging for blended learning, peer support, and mentoring in pediatric and adolescent HIV/AIDS care: A case study in Zimbabwe. Hum Resour Health 2019; 17(1).
- Ce RI: Living well with HIV/AIDS A manual on nutritional care and support for people living with HIV/AIDS.
- Copeland C, Martins R, Thaliffdeen R, Kotsopoulos N, Jarrett J and Chaudhari P: The HIV epidemic in the united states–epidemiological projections and public economic impact of achieving zero transmission Goals. Clin Outcomes Res 2025; 17: 755–69.
- Basta D, Latinovic OS and Silvestri G: Potential Advantages of a Well-balanced Nutrition Regimen for People Living with Human Immunodeficiency Virus Type -1. J AIDS HIV Treat 2024; 6(1): 11–27.
- Fathima AS, Madhu M, Udaya Kumar V, Dhingra S, Kumar N and Singh S: Nutritional Aspects of People Living with HIV (PLHIV) Amidst COVID-19 Pandemic: an Insight. Current Pharmacology Reports. Springer Science and Business Media Deutschland GmbH 2022; 8: 350–64.
- Garg S, Bebarta KK and Tripathi N: The Ayushman Bharat Pradhan Mantri Jan Arogya Yojana (AB-PMJAY) after four years of implementation – is it making an impact on quality of inpatient care and financial protection in India? BMC Health Serv Res 2024; 24(1).
- Gashema P, Ndahimana F, Saramba E, Musafiri T, Ishimwe E and Iradukunda PG: Undetectable = Untransmittable (U = U): insights from people living with HIV attending health facilities in Rwanda. BMC Public Health 2025; 25(1).
- Georgiadis N, Katsimpris A, Halkitis PN, Kaba E, Tzanakaki G and Vassilakou T: Undetectable = Untransmittable: A Cross-Population Systematic Review and Meta-Analysis on Awareness and Acceptance. Pathogens. Multidisciplinary Digital Publishing Institute (MDPI) 2025; 15.
- Health Organization W. World report on vision.
- Karan A, Negandhi H, Kabeer M, Zapata T, Mairembam D and De Graeve H: Achieving universal health coverage and sustainable development goals by 2030: investment estimates to increase production of health professionals in India. Hum Resour Health 2023; 21(1).
- Koni K, Chaudhuri S, Tarugu J, Udayasree K and Hema K: HIV care policy in India. J Fam Med Prim Care 2022; 11(5): 1648–57.
- Makurumidze R: Experiences and lessons learnt from the hiv treat all pilot phase implementation in zimbabwe. HIV/AIDS - Res Palliat Care 2021; 13: 823–8.
- Miller A, Crossland MD, Macnaughton J and Latham K: The usefulness of a wearable electronic vision enhancement system for people with age-related macular degeneration: a randomized crossover trial. Transl Vis Sci Technol 2025; 14(9).
- Naif HM: Pathogenesis of HIV infection. Infect Dis Rep 2013; 5(1): 26–30.
- Okesanya OJ, Ayeni RA, Amadin P, Ngwoke I, Amisu BO and Ukoaka BM: Advances in HIV Treatment and Vaccine Development: Emerging Therapies and Breakthrough Strategies for Long-Term Control. AIDS Research and Treatment. John Wiley and Sons Ltd 2025.
- Rezazadeh L, Ostadrahimi A, Tutunchi H, Naemi Kermanshahi M and Pourmoradian S: Nutrition interventions to address nutritional problems in HIV-positive patients: translating knowledge into practice. J of Health, Popul and Nutrit Bio Med Central Ltd 2023; 42.
- Sharma RS, Rohatgi A, Jain S and Singh D: The Ayushman Bharat Digital Mission (ABDM): making of India’s Digital Health Story. CSI Trans ICT [Internet]. 2023 Apr [cited 2026 Apr 28]; 11(1): 3–9. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10064942/#Abs1
- Tumwebaze M, Rubaihayo J and Harold M: Appraisal of Existing HIV/AIDs Prevention and Control Measures and Presentation of Innovative Strategies to End HIV/AIDS Epidemic by 2030. Open J Epidemiol 2023; 13(03): 178–94.
- Verma R, Khanna P, Prinja S, Rajput M and Arora V: The national programme for control of blindness in India. Australasian Medical Journal. Australasian Medical Journal Pty Ltd 2011; 4: 1–3.
How to cite this article:
Dar IA, Kushwaha S, Sharma T and Sing RK: “Transforming public health in India: a review of technological innovations across national health programs”. Int J Pharmacognosy 2026; 13(6): 553-62. doi link: http://dx.doi.org/10.13040/IJPSR.0975-8232.IJP.13(6).553-62.
This Journal licensed under a Creative Commons Attribution-Non-commercial-Share Alike 3.0 Unported License.
Article Information
4
553-562
686 KB
124
English
IJP
Imran Ali Dar, Satpal Kushwaha *, Tanya Sharma and Ranjan Kr. Singh
Faculty of Pharmaceutical Sciences, Mewar University, Gangrar, Chittorgarh, Rajasthan, India.
rxsingh41800557@gmail.com
06 May 2026
14 May 2026
26 May 2026
10.13040/IJPSR.0975-8232.IJP.13(6).553-62
01 June 2026