


GILBERT’S SYNDROME- A CASE WITH INTERPRETATION AND MANAGEMENT IN UNANI MEDICINE
HTML Full TextGILBERT’S SYNDROME- A CASE WITH INTERPRETATION AND MANAGEMENT IN UNANI MEDICINE
Shabnam Ansari * 1, Fasihuzzaman 1, Mohammad Akhtar Siddiqui 1, Sadia Nikhat 2 and Shafia Mushtaq 1
Department of Moalejat (Unani Medicine) 1, Department of Preventive and Social Medicine 2, Faculty of Medicine (U), Jamia Hamdard, New Delhi - 110062, Delhi, India.
ABSTRACT: Background: Gilbert’s syndrome (GS) is the most common form of congenital, non haemolytic, mild unconjugated hyperbilirubinaemia. Familial cases linked with mutation in enzyme UDP glucuronosyl transferase 1 producing decreased conjugation of bilirubin which accumulates in the form of unconjugated bilirubin. Hyperbilirubinaemia is mild (<6 mg/dl) while liver enzymes & histology are always found normal. It is clinically characterized by vague symptoms like loss of appetite, abdominal pain, weight loss and mild Jaundice. A review of Unani literature showed disease similarity clinically with Su-e-Mizaj Jigar Har Yabis, with dominating features of Safra (yellow bile). Material and Methods: We report our experience with such a case of GS by validated integrative assessment and management with Unani medicine e.g. Arqayat (Makoh+Kasni+Biranjasif), Jigreen, Sharbat-e-Bazoori and Majoon Dabid-ul-Ward along with a short review of literature. Results were analyzed based on clinical and LFT outcomes. Results: Significant symptomatic relief was achieved over 5 weeks of treatment. Bilirubin levels normalized but rose after 5 weeks. Literature review showed disease similarity with Su-e-Mizaj Har Yabis Sadaa which under the aggravating factors progressed to Su-e-Mizaj Har Safrawi. Conclusion: As single abnormal gene in the GS runs in the families & leads to reduced enzymatic expression. This decreases conjugation of unconjugated bilirubin and ultimately unconjugated hyperbilirubinaemia. Thereby normal levels of bilirubin were achieved for concise period of time with symptomatic relief which proves the effectiveness of Unani medicine in GS but establishment of the therapy needs planned study on multiple patients.
| Keywords: |
Unani medicine, Gilbert’s syndrome, Complementary medicine, Graecoarab medicine, Temperament, Unconjugated hyperbilirubinaemia and UDP glucuronosyl transferase
INTRODUCTION: Gilbert’s Syndrome (Su-e-Mizaj Har Safrawi) is the most common form of congenital, non-hemolytic, 2 mild unconjugated hyperbilirubinemia 1, 14 found in 2-19% of population 15, 16.
Familial cases are linked with a mutation in promoter region of enzyme UDP glucuronosyl-transferase 1 (UGT1) 2, 12, 13 leading to reduced enzyme expression. This results in decreased conjugation of bilirubin which accumulates in the form of unconjugated bilirubin.
Hyperbilirubinaemia is mild (>6 mg/dl) 2 while liver enzymes& histology remains normal. The disease is characterized by vague symptoms like fatigue, concentration difficulty, loss of appetite, abdominal pain, weight loss, itching without rashes and mild Jaundice which may appear under the conditions of exertion, stress, fasting, alcohol use, infection 1, 10 and menstruation 17. A review of Unani literature showed disease similarity with Su-e-Mizaj Har Yabis (S. Bilirubin T˂2.5mg/dl) which has a similar clinical presentation with dominating features of Safra (Yellow bile) 6, 8. While the symptomatic cases of GS (cases presented with clinical jaundice, pain at the liver area, nausea, bilious vomiting, and fever) 7, 9 revealed similar clinical features like Su-e-Mizaj Har Safrawi (S. Bilirubin T>2.5 mg/dl in which jaundice appear).
Diagnostic Criteria: 3
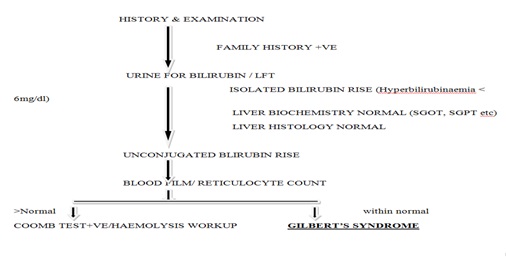
FIG. 1: DIAGNOSTIC CRITERIA
MATERIAL AND METHODS:
Case Study: A young 29 yrs. old Indian, married male admitted on 1st Nov 2013 from Medicine OPD of Majeedia Unani Hospital with complains of 1) Dark Urine, 2) moderate pain in upper abdomen, 3) heaviness in the abdomen after taking a meal, 4) decrease appetite and 5) loose motions 5-6 times per day from 3weeks. History revealed repeated episodes of jaundice starting from 10 yrs of age and level of bilirubin in recent attacks was not more than 6 mg/dl. The positive family history of jaundice was present in grandmother, mother, and his baby. Upon Clinical examination the patient was conscious; vitals were stable, no pallor, and no icterus. Upon per abdominal examination live was palpable with little epigastric tenderness and other system were appeared normal. The initial evaluation is done with the following investigations dated2nd November 2013 given in Table 1 below.
Unani Treatment: Treatment was given under the Unani paradigms with following drugs e.g. Arq Makoh (Aquous extract Solanum nigrum) 50 ml+Arq Kasni (Cichorium intybus) 50 ml+Arq Biranjasif (Achillea millefolium ) 50 ml, combined and 150 ml given b.i.d, Jigreen, 15 ml t.i.d 19, Sharbat-e-bazoori 20 ml, b.i.d 20 and Majoon Dabeed-ul-ward, 7 gm b.i.d 18.
Outcome Measures: Clinical Symptoms and LFT were analyzed after 1, 2, 3, 4, and 5 weeks of treatment.
RESULTS: The patient got an excellent relief in pain and heaviness in the upper abdomen (assessed by visual analog scale) appetite turned out better, and loose stool subsided completely. Effect on symptoms is shown below in Table 2.
TABLE 1: INVESIGATION
| Investigation | Value |
| Hemoglobin | 13.6% |
| Total leucocyte count | 6, 700 cmm |
| Differential leucocyte count | Polymorphs 40, Lymphocyte
46 Eosinophils 6, Basophils 3 |
| Platelet count | 1.2 lakhs |
| ESR | 15 mm per hr |
| Serum bilirubin (total) | 2.3 mg/dl |
| Serum bilirubin (Indirect) | 1.2 mg/dl |
| SGPT | 29 IU/ ml |
| SGOT | 32 IU/ ml |
| Alkaline phosphatase | 128 IU/ ml |
| HbsAg | nR |
| HCV | nR |
| ANA | Negative |
| Kidney function test (KFT) | WNL |
| Reticulocyte count | 1.9 (WNL) |
| Sonography abdomen | Normal study |
TABLE 2: EFFECT OF TREATMENT ON SYMPTOMS
| Symptoms | Admission | After 1st week | After 2nd week | After 3rd week | After 4th week | After 5th week |
| Pain in abdomen (Visual analogue scale) | 5 | 3 | 1 | 0 | 0 | 0 |
| Loss of appetite | Severe anorexia | mild | Normalized | Normal | Normal | Normal |
| Loose stools | 6 loose stools
per day |
1 loose stool per day | Normalized | Normal | Normal | Normal |
| Heaviness in the abdomen after a meal | Present with regurgitation | Present mildly | No heaviness | No heaviness | No heaviness | No heaviness |
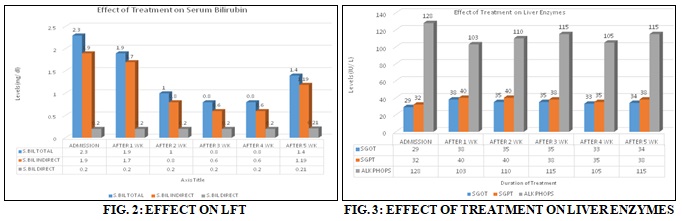
Effect of five weeks of treatment on serum bilirubin and liver enzymes are given in Fig. 2 and 3 below. No adverse events were observed during and after treatment.
DISCUSSION: Majoosi, Avicenna (1037 AD) stated the liver’s normal temperament (Tabyii Mizaj), a hot (Haar) one. The hot temperament could be due to the predominance of either sanguine (Damwi) or bilious (Safrawi) humor. People with normal bilious temperament produces a higher amount of biliary secretions 6, 8. Familial linked cases of GS has the abnormal gene which is not the normal (Tabyii Mizaj) concerning other siblings and individual of a particular group. So, calling the term Su-e-Mizaj (abnormal temperament) for the individual of GS seems much reliable. In Unani literature, Su-e-Mizaj Har Yabis has similar clinical features like GS with dominating features of Safra (Azam khan) 7, 9.
In GS, jaundice and other symptoms such as fatigue, concentration difficulty, loss of appetite, and abdominal pain appear under the condition of exertion, stress, fasting, and infection. So, these symptomatic cases with clinical jaundice cannot be put under Su-e-Mizaj Har Saada. So correlating such cases of GS with Su-e-Mizaj Har Safran which present classical clinical features of jaundice (S. Bil T>3mg/dl in which jaundice appear) will be somehow rational. This states that Su-e-Mizaj Har Saada under aggravating conditions progressed to Su-e-Mizaj Har Safrawi with derangement in both quality and quantity of bilious humor. We treated our case with Jigreen, which has proven effects on anorexia, pain in the abdomen, nausea and vomiting, probably the cause for symptomatic relief in our case. Jigreen has also reduced bilirubin levels and improved other biochemical markers S. A. Tamanna et al., assumed to be the cause for the transient decrease in bilirubin levels.
According to the European monograph, traditionally Chicory (Kasni) has been used for the relief of symptoms related to digestive disorders such as a feeling of abdominal fullness, flatulence, loss of appetite and slow digestion 21. Chicory also exhibited analgesic activity in mice in the hot plate and tail-flick tests 22. Majoon Dabeed-ul-ward is a compound formation of Unani medicine which contains Rosa damescene (Rose) as the main drug, documented as hepatoprotective Avicenna, 1037 AD. Sharbat Bazoori is a Diuretic for evacuation of yellow bile (Safra) Azam Khan 7. So, treatment with Unani Medicine reported significant symptomatic relief, but on LFT, a little decrease in the level of bilirubin was achieved for short period.
CONCLUSION: Proved the symptomatic effects of Unani medicine in GS but after 5weeks bilirubin levels rose again, somehow proved familial linked reduced enzymatic expression 1 but accurate results need planned study on multiple subjects.
ACKNOWLEDGEMENT: We appreciate the cooperation of the patient and the Library of Faculty of Medicine (Unani), Jamia Hamdard, New Delhi, India.
FINANCIAL DISCLOSURE: Conflict of Interest: None declared.
SOURCE OF SUPPORT: Nil
REFERENCES:
- Ghany M and Hoofnagle JH: Liver and biliary tract disease. In Harrison Principle of Internal Medicine, Edition 15th, Volume 2nd, 1718-19.
- Mahdi AS and Elameer MS: psychiatric bulletin, http://pb.rcpsych.org/letters/submit/pbrcpsych;22/9/566
- Chapman RW, Collier JD and Hayes PC: Liver and biliary tract disease. In Davidson Principles and practice of Medicine, Edition 20th, 945-946.
- Black B and Billing BH: The New England Journal of Medicine 1969; 280: 1266-1271. www.nejm.org/doi/full/ 10.1056/nejm196906052802303, Medline web of Science (Medline).
- Kapla M: Gilbert’s syndrome and glucose-6-phosphate dehydrogenase deficiency: a dose-dependent genetic interaction crucial to neonatal hyperbilirubinemia, Vol. 2, 12128-12132 www.pnas.org/content/94/22/12128 (PNAS).
- Majoosi AI: A Kamil-us-Sana [G.H. Kantoori, Trans], New Delhi, Idarah Kitabus Shifa Publishing; Part 38th, Vol 1 & 2, 2010: 440.
- Khan HA and Azam AA: [H. Kabiruddin, Trans], New Delhi, Aijaz Publishing, 2010: 146.
- Sina I: (Avicenna) and Fit-Tibb AQ: [G.H. Kantoori, Trans], New Delhi, Aijaz Publishing; Vol. 3rd, Part 1, 2010: 854.
- Karshi MH and Hikmat J: New Delhi Aijaz Publishing, Vol. 2, 2011: 799-800.
- Gilbert’s disease, www.nlm.nih.gov/medlineplus /ency/ article/000301.htm, Medline Plus.
- Gilbert’s syndrome, Genetic and rare disease information center (GARD), NIH, and raredisease.info.nih.gov/gard /6507/ Gilbert’s’s’ s_syndrome/resources/1.
- Gilbert’s syndrome, Online Mendelian Inheritance of Man (OMM).2009; http://www.ncbi.nlm.nih.gov/omim/143500. [Accessed 5/2/2011].
- Sugatani J, Yamkawa K, Yoshinari K, Machida T, Takagi H, Mori M, Kakizaki S, Sueyoshi T, Negishi M and Miwa M: Identification of a defect in the UGT1A1 gene promoter and its association with hyperbilirubinemia. Biochem Biophys Res Commun 2002; 292: 492-497. [ Pub Med; 11906189, related citations] [Full Text; Elsevier Science].
- Bosma: The genetic basis of the reduced expression of bilirubin UDP-glucoronyl transferase 1 in Gilbert’s’s syndrome. New Eng J Med 1995; 333: 1171-1175. [PubMed; 7565971, related citation] [Full text: Atypon].
- Clarke DJ: Genetic Defect of the UDP-glucuronosyl-transferase-1 (UGT1) gene that causes familial non-hemolytic unconjugated hyperbiliru binaemias, 1997; 266 (1): 63-74. PMID; 9435989 [PubMed-indexed for MEDLINE] related citation].
- Owens D and Evans J: Population studies on Gilbert’s Syndrome. J Med Genet 1975; 12: 152-156. [PubMed; 1142378, related citation.]
- Schmid R: Gilbert’s Syndrome: a legitimate genetic anomaly? (Editorial), New Eng J Med 1995; 333: 1217-1218. [PubMed: 7565981, related citation] [Full text: Atypon].
- Ward MD: Introduction of Majoon, National Formulary of Unani Medicine, Part 65: Part 5, 2008: 90-91:
- Jigreen, Hamdard web, www.hamdard.in/ products.php? pid=8&pN=Jigreen
- Sharbat-e-bazoori, www.hamdard.in/products. php?. ..Sharbat %20Bazoori
- European Medicines Agency: Community herbal monograph on Cichorium intybus, radix. EMA/HMPC/ 121816/2010, 2012.
- Wesołowska A, Nikiforuk A, Michalska K, Kisiel W and Chojnacka-Wójcik E: Analgesic and sedative activities of lactucin and some lactucin-like guaianolides in mice. Journal of Ethnopharmacology 2006; 107(2): 254-258. [PubMed]
- Tamanna SA: Effect of Jigreen on Patients suffering from hepatitis B. In Proceeding of the National Seminar on Research Methodology in Unani Medicine 1995; 111-116.
How to cite this article:
Ansari S, Fasihuzzaman, Siddiqui MA, Nikhat S and Mushtaq S: Gilbert’s syndrome- A case with interpretation and management in Unani medicine. Int J Pharmacognosy 2015; 2(2): 98-01. doi link: http://dx.doi.org/10.13040/IJPSR.0975-8232.IJP.2(2).98-01.
This Journal licensed under a Creative Commons Attribution-Non-commercial-Share Alike 3.0 Unported License.
Article Information
8
98-101
610
2982
English
IJP
S. Ansari *, Fasihuzzaman, M. A. Siddiqui, S. Nikhat and S. Mushtaq
Department of Moalejat (Unani medicine), Faculty of Medicine (U), Jamia Hamdard, New Delhi, Delhi, India
drshabnamansari.md@gmail.com
27 December 2014
19 January 2015
27 January 2015
http://dx.doi.org/10.13040/IJPSR.0975-8232.IJP.2(2).98-101.
01 February 2015