


UNVELLING THE ANTI-DIABETIC EFFICACY OF A TRADITIONAL HERB PARADIGM SHIFT IN DIABETIC MANAGEMENT
HTML Full TextUNVELLING THE ANTI-DIABETIC EFFICACY OF A TRADITIONAL HERB PARADIGM SHIFT IN DIABETIC MANAGEMENT
A. Kumar, Hrathaur * and S. Mukhopadhyay
College of Pharmacy, Shivalik Campus, Sihniwala, Shimla Bypass Road, Dehradun, Uttarakhand, India.
ABSTRACT: The global health crisis posed by diabetes mellitus, characterized by chronic hyperglycemia, requires innovative strategies to address its increasing prevalence and associated complications. Traditional medicine, with its holistic healing principles, offers a promising avenue. This review explores a groundbreaking study that focuses on a polyherbal formulation for managing diabetes, representing a change in perspective for the treatment of this disease. Considering the concerning prevalence of diabetes on a global scale, it is imperative to explore alternative treatments. Traditional polyherbal formulations, rooted in ancient wisdom, are attracting growing attention. These formulations combine various plant-based ingredients, harnessing their synergistic potential for managing diseases. This review offers insights into the pre-clinical investigation of a specific polyherbal formulation, shedding light on its potential for effectively managing diabetes. In-vitro and in-vivo are conducted to evaluate the formulation's ability to lower blood sugar and improve sensitivity to insulin. Additionally, comprehensive assessments are carried out to ensure its safety and identify any potential side effects. The results demonstrate the promising anti-diabetic effects of this traditional polyherbal, suggesting the possibility of a safer and more accessible alternative to conventional pharmaceuticals. This paradigm shift highlights the importance of integrating traditional knowledge with rigorous scientific approaches, potentially revolutionizing the management of diabetes. The review paper emphasizes the potential of traditional polyherbal formulations as a comprehensive strategy for managing diabetes, offering viable and secure alternatives to conventional medications.
Keywords: Diabetes mellitus, Polyherbal, Antidiabetic, Herbal medicine, Conventional, Holistic
INTRODUCTION: The field of herbal medicine has experienced a surge in popularity due to its natural origins and limited adverse reactions consequently, there has been a significant rise in the occurrence of this field.
Diabetes mellitus, a collection of metabolic conditions defined by elevated levels of sugar in the blood due to insufficient insulin production or an ineffective insulin response, is a widespread metabolic condition that affects 2.8% of the worldwide populace. Forecasts suggest that this amount will increase to 5.4% by the year 2025. Hyperglycemia associated with diabetes can lead to damage in several organs, including the heart, blood vessels, kidneys, nerves, and eyes. In the treatment of diabetes, herbal folk medicine has been utilized, known for its antioxidant properties and minimal side effects 1. More than 800 plants are said to have antidiabetic qualities in historical literature. Their purported Ethnopharmacological studies reveal that over 1200 plants are employed in traditional medicine due to ability to lower blood sugar levels 2. Ayurvedic remedies for diabetes improve the body's capacity to process food by boosting gastric secretions (one of the Rasas). They are considered easy for the body to assimilate due to their lightweight (Laghu) nature, and their dry (Ruksha) qualities help reduce overall bodily fluid production, including perspiration and urine 3. The Indian material medica lists various substances (dravyas) that have been documented as effective in the treatment of Madhumeha (diabetes) 4. Consequently, it is imperative to conduct scientific assessments and screenings of these plants through pharmacological tests and chemical investigations 1.
Pathophysiology of Diabetes: Diabetes mellitus comprises type 1 (IDDM) and type 2 (NIDDM) diabetes:
Type 1 Diabetes (IDDM):
- Autoimmune (Type 1A) or idiopathic (Type 1B) destruction of pancreatic β-cells.
- Complete insulin insufficiency.
- Usually affects young adults and children.
Type 2 Diabetes (NIDDM):
- Insulin resistance and reduced responsiveness to insulin.
- Commonly observed in overweight adults over 40.
- Disturbed carbohydrate and fat metabolism.
Common Pathophysiological Factors:
- Free Radicals: Implicated in diabetes development and complications, causing damage to DNA, proteins, lipids, and other substances found in cells.
- Lipid and Protein Abnormalities: Key contributors to diabetic complications.
- Reactive Oxygen Species (ROS): Generated in various tissues and contribute to insulin intolerance.
- Oxidative Stress: Occurs concurrently with reduced antioxidant levels, leading to harmful effects.
- Plant-Based Antioxidants: Some natural compounds, like vitamins C and E, may mitigate oxidative stress in diabetes 5.
Types of Diabetes:
Type I: Diabetes Mellitus: This happens when the kidneys are unable to generate adequate insulin to fulfill the physical structure requirements. The immune system targets and kills the pancreatic beta cells in response to a trigger, such as a disease or stressful event. Consequently, the pancreas ceases to produce insulin. First and foremost, insulin injections are used as a type I diabetic therapy. Must endure each day. Another name for this kind of diabetes is diabetes mellitus with insulin reliance (IDDM). Type I arises abruptly in early life or adolescence 6.
Type II: Diabetes Mellitus: Condition known as "insulin resistance." Type II diabetes is significantly more widespread than Type I and comprises approximately 90% of all diabetes cases. There is a substantial genetic inclination for Type II diabetes, and other factors that contribute to risk include advancing age, obesity, and a sedentary lifestyle. This type of diabetes is often referred to this occurs when the pancreas produces insulin, but the cells are incapable of using it efficiently, and primarily impacts individuals over 40 years of age, especially those who are overweight 6.
Gestational Diabetes Mellitus: Glucose intolerance, which manifests itself during pregnancy, is a condition that warrants attention due to its potential to complicate the gestational period resulting in adverse outcomes for both the mother and fetus. Therefore, the clinical identification of this condition assumes great significance. Although gestational diabetes can be effectively managed, it necessitates diligent medical oversight throughout the duration of the pregnancy. It is noteworthy that a considerable proportion, ranging from 20% to 50% of women affected by this condition subsequently develop type 2 diabetes later in life 6.
Other Particular forms of Diabetes: Maturity onset diabetes of the young is identified by reduced insulin production and typically involves low-level or nonexistent insulin resistance, which leads to the early appearance of hyperglycemia. A genetic deficiency in converting proinsulin into insulin results in mild hyperglycemia. The pathological characteristics. The development of diabetes mellitus can be linked to the following factors:
- Reduced glucose consumption by the body's cells, leading to a rise in blood sugar levels ranging from 300 to 1200 mg/dL.
- Enhanced mobilization disrupting normal metabolism of fat and causing the Cholesterol buildup in artery walls is a contributing factor, ultimately contributing to atherosclerosis.
- Depletion of protein in body tissues, resulting in a scarcity of protein within the tissues 6.
Prevalence of Diabetes around the World: Diabetes, being a metabolic condition, is a significant health concern affecting populations in both advanced and emerging nations. According to data from around the world, the worldwide diabetes prevalence is currently approximated at 4.6%, impacting around 152 million individuals. It is projected to rise to approximately 333million individuals by 2025. Recent findings suggest a more concerning trend, with the global prevalence reaching 6.6% in 2010, affecting around 285 million individuals, and this figure anticipates to climb to 7.8% (approximately 438 million people) by 2030. Diabetes rates vary widely globally, affecting mainly developing countries and lower socioeconomic groups. By 2010, it was projected to account for 11.6% of global healthcare spending, with costs expected to reach $490 billion by 2030, according to the IDF. While more prevalent in males, there are actually more reported cases of women living with diabetes 7. A significant rise in the percentage of individuals over the age of 65 who are affected by diabetes 8. Research has revealed a startling increase in the incidence of diabetes in India 9.
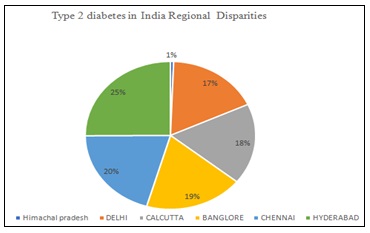
GRAPH 1: THE DIABETES EPIDEMIOLOGY STUDY GROUP IN INDIA 11, 12
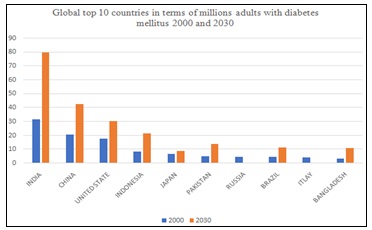
GRAPH 2: LIST OF NATIONS WITH THE GREATEST PROJECTED DIABETES CASES BETWEEN 2000 AND 2030. ADAPTED FROM BAYNES HW 13
As per the World Health Organization (WHO), India had 31.7 million individuals with diabetes in the year 2000, and this figure is projected to escalate to 79.4 million by the year 2030 8. India holds the distinction of having the highest number of diabetes cases worldwide and is often referred to as the "diabetes capital of the world." Research underscores a notable diabetes prevalence rising with age, particularly among urban individuals with sedentary habits 10.
Herbal Medicines: The traditional Indian Ayurvedic medicine system emphasizes the use of natural products to encourage a healthy lifestyle and the prevention of unnecessary illnesses. This age-old medical approach is renowned for employing a range of herbal remedies to address various health imbalances. The core principle in Ayurveda is not only to restore a disease-free body but also to prevent its reappearance 14.
Herbal medicine systems from various regions across the world have utilized polyherbal formulations for their diverse and multifaceted pharmacological effects 15. The majority of Ayurvedic formulations are based on herbs, which are utilized as decoctions, infusions, tinctures, and powders. Ayurvedic drug formulation is based on two principles, as stated in Ayurvedic treatises such as Charaka Samhita and Sushruta Samhita: (a). Use as a single medication, and (b). Utilizing more than two medications. Polyherbal formulations are those that contain two or more herbs 16.
Rationale of Polyherbal Formulation: PHF has recently been more well-known all over the world since it offers a number of benefits that allopathic medicines do not have.
Firstly, PHFs have a reputation for being highly effective for a wide range of illnesses. As previously indicated, the presence of various phytoconstituents contributes to the effects of herbal medications on health, and the presence of suitable herbals in PHFs further amplifies the benefits. PHF has been the subject of several studies to date, all of that have been printed in foreign journals to assess their efficacy. For example, a number of anti-diabetic PHFs, including Diahar Diabet, Diasol Dianex, DRF/AY/5001, Diashis, Diabrid, Diakyur, Diasulin, and others, have been reported by Srivastava et al. in their study and are verified to have effects that are consistent with those of mainstream allopathic drugs 17. The efficacy and positive results of the therapy effects of herbal medications on health driving the application of herbal medicine, according to a UK statistical research 18.
Polyherbal formulations (PHFs) often offer a broad treatment range with a favorable risk-to-benefit ratio. For instance, Diakyur, a hypoglycemic PHF, showed no toxicity in animals even at high doses of 12800 mg/kg orally. It's considered safe for long-term use at 1600 mg/kg 19. orally and exhibits antioxidant and hypoglycemic effects. This contrasts with sulfonylureas known for their limited therapeutic index 20.
Usually, herbal treatments, when properly administered, cause less adverse effects in comparison to conventional medications. While Modern medications are made to be as effective as possible, they often bring about problems like insomnia, nausea, and more. For instance, patients with rheumatoid arthritis may experience gastrointestinal and renal issues with standard drugs. Ayurvedic treatments offer a less troublesome alternative. Research has shown that one year of Ayurvedic treatment can benefit rheumatoid arthritis patients without harming their organs 21. Furthermore, according to Jawla et al., none of the 500 participants in their survey reported experiencing adverse effects from herbal remedies. Moreover, 48% of them showed a preference for the Ayurvedic method in treating common ailments. The acceptance of this medicinal system by the public seems to be influenced by considerations regarding potential side effects 22, 23.
Advantages of Polyherbal Formulation Over Allopathy:
Natural Healing: Polyherbal formulations do not disrupt the body's inherent self-healing capabilities; instead, they enhance the body's natural healing mechanisms, expediting the recovery process. This enhancement assists the body in maintaining an optimal internal environment, which is crucial for effective healing.
Ongoing Benefits: Many polyherbal remedies come with dietary, relaxation, and exercise recommendations that enhance the treatment's effectiveness. These nutritional and lifestyle guidelines enable the body to adapt to the therapy more rapidly, establishing healthier habits for the patient.
Enhanced Immunity: Polyherbal treatments bolster the immune system by promoting the body's innate healing processes and addressing detrimental habits that contribute to illness.
Metabolism and Nutrition: A more robust immune system, combined with a balanced diet and lifestyle, results in enhanced metabolism. Consequently, this results in increased absorption of vitamins from the diet.
Minimal Side Effects: Herbal remedies typically have minimal adverse effects and contraindications when utilized as directed and under the supervision of an experienced practitioner 16, 24.
TABLE 1: ANTIDIABETIC ACTIVITY REPORTED ON FOLLOWING PLANTS
| Plant name | Traditional/common name | Part used | The anti-diabetic effect and additional noteworthy effects |
| Acacia arabidca (Leguminosae) | Guar gum, gum Arabic | Seeds | Hypoglycemia: incite the release of insulin from pancreatic B-cells |
| Anethum graveolens
(Umbellierae) |
Dill | Leaves | Antioxidant, hypoglycemic, and drop in serum insulin levels |
| Areca catechu(Palmae) | Betalnut, supari | Fruits | Hypoglyceic |
| Azadirachta indica
(Mellaceae) |
Neem | Leaves, Seed | Antioxidant, antihyperglycemic, and hepatoprotective |
| Beta vulgaris
(Chenopodiaceae) |
Chukkander, beetroot, or
Garden beet |
Root | Enhanced ability to tolerate glucose |
| Brassica juncea
(Brassicaceae) |
Mustard greens, Indian mustard, Chinese mustard, | leaves | Hypoglycemic, antioxidant |
| Butaemonosperma
(Papillionaceae) |
Palasa,flame of the forest) | Bark, leaves, flower | Antihyperglycemic and hypoglycemic antioxidant and thyroid-inhibiting properties |
| Cassia auriculata (Caesalpiniaceae) | Ranawara" or avaram", avaram senna | Leaves, flowers | A-glucosidase inhibitory effect, antihyperglycemic and hypolipidemic action |
| Cinnamomum osmophloeum (Lauraceae) | Pseudocinnamomum" or indigenous cinnamon | Leaves
|
increased production of adinopectin and insulin-signaling pathway activation |
| Cinnamomum verum (Lauraceae) | True cinnamon, ceylon cinnamon | Leaves
|
Human pancreatic a-amylase inhibition is concentration-dependent. |
| Citrus sinensis (Rutaceae)
|
Sweet orange
|
Peel of fruit
|
antiperoxidative, antihyperglycemic, and cardioprotective reduced cardiovascular risk factors and hypoglycemia |
| Coscinium fenestratum (Menispermaceae) | -
|
Stem
|
Antidiabetic, hypolipidemic
|
| Curcuma longa (Zingiberaceae) | Turmeric
|
Rhizome
|
Human pancreatic a-amylase inhibition is concentration-dependent. |
| Emblica officinalis (Euphorbiaceae | Amla, dhatriphala
|
Fruit
|
Hypoglycemic, lipid peroxidation-reducing, antioxidant, and gastroprotective |
| Ficus bengalensis (Moracese)
|
Bur", banyan
|
Aerial root, stem bark | Antioxidant-dependent, concentration-dependent suppression of human pancreatic a-amylase in hypoglycemia |
| Gymnema sylvestre (Apocynaceae) | Gurmar, gymnema | Leaf | It lowers blood sugar by raising the body's insulin production. |
| Psidium guajava, | Guava,lemon guava | leaf | Lowers plasma glucose level |
| Camellia sinensis (theaceae) | Green tea | leaves and leaf buds | Hypoglycemic activity |
| Syzygium cumini (Myrtaceae) | Jamun fruits | seed | Lower blood sugar while simultaneously blocking the alpha glucosidase enzyme. |
| Ocimum sanctum
(Lamiaceae) |
Tulsi | leaf | Hypoglycaemic and hypolipidemic effect |
| Momordica charantia (Cucurbitaceae) | Karela | Seeds, pulp | Reduce blood glucose level |
| Trigonella foenum Grae
(Fabaceae) |
Methi | Seed | Decrease blood glucose concentration |
| Vinca rosea
(Apocynaceae) |
Vinca | ;EAF | Alpha glucosidase inhibitors |
| Murrayakoenigii (Rutaceae) | Daun Kari, Indian Curry Tree, Curry Leaf Tree | Leaf extract | Antidiabetic, antioxidant, Immunomodulatory Activity, |
Scientific Preclinical Evidence:
Azadirachta indica A (Neem): A Studies on indica found that the leaves were more effective than the seeds. In an experiment involving diabetic rats, oral administration of leaf aqueous extract resulted in blood glucose reduction by 3.3% to 11.7% at 200 mg/kg and 38.7% at 300 mg/kg (P < 0.05). Conversely, the seed aqueous extract at 200 mg/rat caused a decrease ranging from 20% to 33.8% (P < 0.05). In another study, the leaf extract significantly increased cholesterol levels compared to the control group, but at high doses, it caused adverse effects like decreased appetite, weight loss, and mortality. Diabetic blood showed delayed clotting times, indicating platelet dysfunction and slow wound healing. Injecting the leaf extract reduced T1DM by 45.4% and T2DM by 60% compared to the control group.
Allium cepa: Pyaj (Hindi) and Onion (English): The first evidence that taking Allium cepa (onion) orally might improve glucose control in diabetics came from Mathew and Augusti in 1975. A. cepa was also shown to have an immediate hypoglycemia impact in self-controlled research with twenty T2D patients. Furthermore, it was discovered to decrease the rise in plasma glucose that occurs two hours after glucose administration by 37%. More recently, it has been shown that giving T1D and T2D patients 100 grams of A. cepa can improve glucose tolerance tests (GTT) and decrease fasting blood glucose (FBG) levels 27.
Aloe vera: Aloe vera is a medicinal plant native to Thailand and is believed to possess properties that can help manage diabetes. In our initial clinical investigation into the anti-diabetic effects of Aloe vera L 28. It has been documented to exhibit hypoglycemic effects by directly reducing blood glucose levels and enhancing insulin sensitivity 29. When alloxanized Mice underwent one experiment. oral administration a 500 mg/kg dosage of aloe, there was no notable decrease observed in their fasting plasma glucose levels 30. However, in the case of chronic oral administration of aloe at the same dose (500 mg/kg), twice daily, there was a significant reduction in fasting plasma glucose (FPG) levels, indicated by a p-value of less than 0.001. This reduction was particularly evident on the 3rd, 4th, and 5th days, with percentage reductions of 30.7%, 32.1%, and 37.7%, respectively. These findings provide confirmation of aloe's reported hypoglycemic properties. During the acute studies, there were no changes in body weight, and no instances of purgation were observed. However, in the long-term researcha small amount of purgation and a decrease in body weight occurred 31.
Curcuma longa (Turmeric): Curcumin, the primary yellow pigment obtained from turmeric, which is the powdered rhizome of the Curcuma longa herb, is known to exhibit a diverse array of effects. It possesses anti-inflammatory, antioxidant, antihepatotoxic, and hypocholesterolemia properties. Furthermore, curcumin is reported to have a positive impact on blood glucose amounts in rats with diabetes 32. The extract from the rhizome of Curcuma longa demonstrated the ability to lower blood glucose levels in experimental rats with induced diabetes. Furthermore, the treatment with Curcumin resulted in significant reductions in the infiltration of macrophages into white adipose tissue, elevated adiponectin synthesis in this tissue, and a decrease in hepatic nuclear factor-kappa B activity, liver hypertrophy, and indicators of liver inflammation. As a result, we can determine that verbally administered Curcumin has the potential to counteract a large number of the metabolic and inflammatory issues connected to obesity, while also improving Glycemic management in rats with diabetes 33.
Emblica officinalis: E. officinalis, a plant with high medicinal value, primarily demonstrates immunomodulatory and immune-enhancing effects. Its pharmacological properties, including antioxidants and anti-inflammatory characteristics, influence the immune system 34. A study administered aqueous amla fruit extract to rats given alloxan to induce diabetes, which led to decreased blood sugar and triglyceride levels. It also improved liver function by normalizing alanine transaminase activity.
E. officinalis leaf extract effectively restored level of antioxidants in diabetes caused by streptozotocin in a dose- reliant way, surpassing glipalamide- tended groupings. The passage rapidly protected against lipid peroxidation, lowering the chance of complications from diabetes through free radical scavenging 35.
Gymnema sylvestre (Gurmar): The word "gymnema" originates from the Hindu word "Gurmar," which means "sugar destroyer." Gymnema is said to have the ability to reduce the body's excess sugar content, especially in those with diabetes mellitus. Known for its strong antidiabetic properties, G. silvestre is used extensively in homeopathic, Ayurvedic, and folk medicine 36. Research indicates that this plant significantly (p < 0.05) reduces high levels of blood glucose, ALT, AST, triglycerides, total cholesterol, LDL-cholesterol, and malondialdehyde in rats with diabetes caused by streptozotocin. Additionally, it exhibits a substantial (p < 0.05) increase in insulin, HDL-cholesterol, and erythrocyte superoxide dismutase levels in diabetic rats. It is interesting because it can fix damaged β-cells, which make insulin 37.
Momordica charantia (Karela): The seeds, fruit pulp, leaves, and entire plant of MC have all been linked to hypoglycemia in normal animals, according to several animal studies 38, 39. MC specifically enhances glucose tolerance 40. and reduces the hyperglycemia that follows a meal in rats Lipolysis and insulin sensitivity can both be improved by MC extract 41, 42. Furthermore, according to certain investigations, MC's hypoglycemic impact was on par with that of oral drugs such tolbutamide 43, propylpropamide, glibenclamide as well Many Studies on biochemistry have shed light on the mechanisms of MC's anti-diabetic effects; stimulation of the A typical one is the AMP-activated protein kinase pathway. Thesa- and g-peroxisome proliferator-activated receptors (PPARa and PPARg), which are essential for controlling lipid and glucose levels, have been suggested in other studies as potentially reducing insulin resistance 44. A short while ago, a protein without zinc that exhibits insulin-like properties was identified in Momordica charantia 45, reminiscent of the concept of 'vegetable insulin' that Baldwa et al. isolated some 30 years ago 46.
Murraya koenigii (Curry Leaves): Murraykoenigii is used to treat diarrhea, as a stimulant, and to control diabetic mellitus. The bark, roots, and leaves have carminative, stomachic, and tonic qualities 47. For the investigation, albino rats weighing 150–250 grams of both sexes were used. Before being employed in the next investigation, these rats were given two to three days to become acclimated to their new surroundings 48. An ethanol-based M. koenigii extract was shown in research to significantly lower blood glucose levels. The decrease was ascribed to M. koenigii's insulin mimetic actions and antioxidant characteristics. Moreover, M. koenigii demonstrated potent antioxidant benefits by raising glutathione (GSH) levels, lowering the homeostasis model assessment (HOMA) insulin resistance score, and lowering malondialdehyde (MDA) levels. All things considered, this study suggests that M. koenigii has antioxidant properties and antidiabetic efficacy in rats 49.
Osmium sanctum: Thirty individuals with Type 2 Diabetes (T2D) experienced a notable alleviation of diabetic symptoms, such as fatigue, polydipsia, and polyphagia, following a three-month regimen of 2 g/day of Osmium sanctum leaf powder. Additionally, in a group of 27 T2D patients, a one-month dietary supplement comprising O. sanctum powder produced an important 21% reduction in fasting blood sugar (FBG), an 11% decrease in glycated protein, an 11% decrease in total cholesterol, a 14% reduction in LDL, a 17% reduction in very VLDL, and a 16% reduction in triglycerides (TG). Confirming these hypoglycemic and hypolipidemic effects, A single-blind, randomized, placebo-controlled study study involving T2D individuals was conducted 49.
Trigonella foenum-graecum (Fenugreek): The T. foenum-graecum fresh seeds were first allowed to dry outside before being processed using a grinder to a powder. Wistar strain albino rats weighing 150–250g were used in the study; they were obtained from the animal house at BCSIR laboratory in Chittagong. Standard laboratory settings were established for these rats, which included a 12-hour photoperiod, with a temporal 24 ± 1°C, along with a humidity level of 55 ± 5%. Prior to the start of the trial, they were kept in galvanized cages with hanging wire mesh, each holding four to six rats. The rats were given access to semi-purified baseline food and unlimited water during the trial, and their care was administered in accordance with accepted ethical standards for using animals in research 50.
Vinca rosea: India has a large distribution of Vinca rosea, both in cultivated and waste regions. At four hours, the water-soluble fraction of the ethanolic extract of Vinca rosea leaves administered orally to normal rats at doses of 100, 250, 500, and 1000 mg/kg caused a significant and dose-dependent decrease in blood sugar, with reductions of 26.22%, 31.39%, 35.57%, and 33.37%, respectively. Additionally, when given at 500 mg/kg, it showed notable anti-hyperglycemic effects 72 hours after the treatment of streptozotocin (STZ) and 3.5 hours before an oral glucose tolerance test (OGTT). Up to an intraperitoneal dosage of 4 gm/kg, no discernible toxic effects or unfavorable behavioral changes were seen 51.
CONCLUSION: Plants have consistently served as a crucial reservoir for discovering novel remedies to address human diseases. Despite the extensive exploration of numerous plants in relation to diabetes, only a limited subset has undergone testing in animal studies and progressed to clinical trials. The plants highlighted in this paper, specifically Azadira chtaindia Allium cepa, Aloe vera, Curcuma longa Momordica charantia, and Trigonella foenum-graecum, Emblica officialsss exhibit clinical evidence supporting their potential antidiabetic effects. Consequently, it appears plausible for healthcare professionals to consider these herbal options, at least as supplementary therapeutic measures, in conjunction with existing hypoglycemic medications to enhance the management of diabetic patients.
ACKNOWLEDGEMENT: Nil
CONFLICT OF INTEREST: Nil
REFERENCES:
- Fatima A, Agrawal P and Singh PP: Herbal option for diabetes: an overview. Asian Pacific Journal of Tropical Disease 2012; 2: 536-44
- Jarald E, Joshi SB, Jain D, Subbulakshmi G and Naik M: Diabetes and herbal medicines indigenous foods in the treatment of diabetes mellitus. Bombay Hospital J 2001; 43(4): 548-61
- Sabu MC and Subburaju T: Effect of Cassia auriculata Linn. on serum glucose level, glucose utilization by isolated rat hemidiaphragm. J Ethnopharmacol 2002; 80.
- Khan V, Najmi AK, Akhtar M, Aqil M, Mujeeb M and Pillai KK: A pharmacological appraisal of medicinal plants with antidiabetic potential. Journal of Pharmacy & Bioallied Sciences 2012; 4(1): 27.
- Shukla A, Bukhariya V, Mehta J, Bajaj J, Charde R, Charde M and Gandhare B: Herbal remedies for diabetes: an overview. International Journal of Biomedical and Advance Research 2011; 2(1): 57-68.
- Colagiuri R: Diabetes: a pandemic, a development issue or both?. Expert Review of Cardiovascular Therapy 2010; 8(3): 305-9.
- Wild S, Roglic G, Green A, Sicree R and King H: Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 2004; 27(5): 1047-53.
- Modak M, Dixit P, Londhe J, Ghaskadbi S and Devasagayam TP: Indian herbs and herbal drugs used for the treatment of diabetes. Journal of Clinical Biochemistry and Nutrition 2007; 40(3): 163-73.
- Gupta A, Gupta R, Sarna M, Rastogi S, Gupta VP and Kothari K: Prevalence of diabetes, impaired fasting glucose and insulin resistance syndrome in an urban Indian population. Diabetes Research and Clinical Practice 2003; 61(1): 69-76.
- Gupta R and Misra A: Type 2 diabetes in India: regional disparities. The British Journal of Diabetes & Vascular Disease 2007; 7(1): 12-6.
- Ramachandran A, Snehalatha C and Kapur A: High prevalence of diabetes and impaired glucose tolerance in India: National Urban Diabetes Survey. Diabetologia 2001; 44: 1094-101.
- Baynes HW: Classification, pathophysiology, diagnosis and management of diabetes mellitus. J Diabetes Metab 2015; 6(5): 1-9.
- Dubey S and Dixit AK: Preclinical evidence of polyherbal formulations on wound healing: A systematic review on research trends and perspectives. Journal of Ayurveda and Integrative Medicine 2023; 14(2): 100688.
- Dubey S and Dixit AK: Preclinical evidence of polyherbal formulations on wound healing: A systematic review on research trends and perspectives. Journal of Ayurveda and Integrative Medicine 2023; 14(2): 100688.
- Kaur M and Valecha V: Diabetes and antidiabetic herbal formulations: an alternative to Allopathy. Eur J Med 2014; 6(4): 226-40.
- Parasuraman S, Thing GS and Dhanaraj SA: Polyherbal formulation: Concept of ayurveda. Pharmacognosy Reviews 2014; 8(16): 73.
- Little CV: Simply because it works better: Exploring motives for the use of medical herbalism in contemporary U.K. health care. Complement Ther Med 2009; 17: 300.
- Joshi CS, Priya ES and Venkataraman S: Acute and subacute toxicity studies on the polyherbal antidiabetic formulation diakyur in experimental animal models. J Health Sci 2007; 53: 245.
- Nazarko L: Nursing in Care Homes. Oxford: Blackwell Science Ltd 2002.
- Krishna KP: The efficacy of Ayurvedic treatment for rheumatoid arthritis: Cross sectional experiential profile of a longitudinal study. Int J Ayurveda Res 2011; 2: 8.
- Jawla S, Gupta AK, Singla R and Gupta V: General awareness and relative popularity of allopathic, ayurvedic and homeopathic systems. J Chem Pharm Res 2009; 1: 105.
- Chatterjee B, Biswas PC and Pancholi J: Health awareness and popularity of alternative medicines among people of Jamnagar town: A cross sectional study. Ayu 2012; 33: 33.
- Cited from http://www.OAWPolicy.com
- Verma S: Formulation and evaluation of anti diabetic polyherbal formulation for the treatment of diabetes.
- Patil SM, Shirahatti PS and Ramu R: Azadirachta indica A. Juss (neem) against diabetes mellitus: A critical review on its phytochemistry, pharmacology, and toxicology. J of Pharmacy and Pharmacology 2022; 74(5): 681-710
- Ghorbani A: Best herbs for managing diabetes: a review of clinical studies. Brazilian Journal of Pharmaceutical Sciences 2013; 49: 413-22.
- Bunyapraphatsara N, Yongchaiyudha S, Rungpitarangsi V and Chokechaijaroenporn O: Antidiabetic activity of Aloe vera L. juice II. Clinical trial in diabetes mellitus patients in combination with glibenclamide. Phytomedicine 1996; 3(3): 245-8.
- Yongchaiyudha S, Rungpitarangsi V, Bunyapraphatsara N and Chokechaijaroenporn O: Antidiabetic activity of Aloe vera L. juice. I. Clinical trial in new cases of diabetes mellitus. Phytomedicine 1996; 3(3): 241-3.
- Ajabnoor MA: Effect of aloes on blood glucose levels in normal and alloxan diabetic mice. Journal of Ethnopharmacology 1990; 28(2): 215-20.
- Suksomboon N, Poolsup N and Punthanitisarn S: Effect of Aloe vera on glycaemic control in prediabetes and type 2 diabetes: a systematic review and meta‐analysis. Journal of Clinical Pharmacy and Therapeutics 2016; 41(2): 180-8.
- Fujiwara H, Hosokawa M, Zhou X, Fujimoto S, Fukuda K, Toyoda K, Nishi Y, Fujita Y, Yamada K, Yamada Y and Seino Y: Curcumin inhibits glucose production in isolated mice hepatocytes. Diabetes Research and Clinical Practice. 2008; 80(2): 185-91.
- Kumar N and Sakhya SK: Ethnopharmacological properties of Curcuma longa: a review. International J of Pharmaceutical Sciences and Research 2013; 4(1): 103.
- Yadav SS, Singh MK, Singh PK and Kumar V: Traditional knowledge to clinical trials: A review on therapeutic actions of Emblica officinalis. Biomedicine & Pharmacotherapy 2017; 93: 1292-302.
- Bhagat M: Indian gooseberry (Emblica officinalis): Pharmacognosy review. Utilisation and Management of Medicinal Plants 2014; 2: 471-87.
- Saneja A, Sharma C, Aneja KR and Pahwa R, Der P Day C, Cartwright T and Provost J: Gymnema sylvestre (Gurmar): A review. Hypoglycaemic effect of Momordica charantia extracts. Planta Med 1990; 56: 426–429.
- Jayasooriya AP, Sakono M and Yukizaki C: Effects of Momordica charantia powder on serum glucose levels and various lipid parameters in rats fed with cholesterol-free and cholesterol-enriched diets. J Ethnopharmacol 2000; 72: 331–336.
- Leatherdale BA, Panesar RK and Singh G: Improvement in glucose tolerance due to Momordica charantia (Karela). BMJ 1981; 282: 1823–1824.
- Chen Q, Chan LL & Li ET: Bitter melon (Momordica charantia) reduces adiposity, lowers serum insulin and normalizes glucose tolerance in rats fed a high fat diet. J Nutr 2003; 133: 1088–1093.
- Chen Q & Li ET: Reduced adiposity in bitter melon (Momordica charanita) fed rats is associated with lower tissue triglyceride and higher plasma catecholamines. Br J Nutr 2005; 93: 747–754.
- Sarkar S, Pranava M & Marita R: Demonstration of the hypoglycemic action of Momordica charantia in a validated animal model of diabetes. Pharmacol Res 1996; 33: 1–4.
- Leung L, Birtwhistle R, Kotecha J, Hannah S and Cuthbertson S: Anti-diabetic and hypoglycaemic effects of Momordica charantia (bitter melon): a mini review. British Journal of Nutrition 2009; 102(12): 1703-8.
- Poovitha S and Parani M: “In-vitro and in-vivo α-amylase and α-glucosidase inhibiting activities of the protein extracts from two varieties of bitter gourd (Momordica charantia L.),” BMC Complementary and Alternative Medicine 2016; 16(1): 185.
- Baldwa VS, Bhandari CM and Pangaria A: Clinical trials in patients with diabetes mellitus of an insulin-like compound obtained from plant source. Ups J Med Sci 1977; 82: 39–41.
- Khan F, Sarker MM, Ming LC, Mohamed IN, Zhao C, Sheikh BY, Tsong HF and Rashid MA: Comprehensive review on phytochemicals, pharmacological and clinical potentials of Gymnemasylvestre. Frontiers in Pharmacology 2019; 10: 1223.
- Bhandari PR: Curry leaf (Murraya koenigii) or cure leaf: review of its curative properties. Journal of Medical Nutrition and Nutraceuticals 2012; 1(2): 92.
- Yadav S, Vats V, Dhunnoo Y and Grover JK: Hypoglycemic and antihyperglycemic activity of Murraya koenigii leaves in diabetic rats. Journal of Ethnopharmacology 2002; 82(2-3): 111-6.
- Khan F, Sarker MM, Ming LC, Mohamed IN, Zhao C, Sheikh BY, Tsong HF and Rashid MA: Comprehensive review on phytochemicals, pharmacological and clinical potentials of Gymnema sylvestre. Frontiers in Pharmacology 2019; 10: 1223.
- Ghorbani A: Best herbs for managing diabetes: a review of clinical studies. Brazilian Journal of Pharmaceutical Sciences 2013; 49: 413-22.
- Mowl A, Alauddin M, Rahman M and Ahmed K: Antihyperglycemic effect of Trigonella foenum-graecum (fenugreek) seed extract in alloxan-induced diabetic rats and its use in diabetes mellitus: a brief qualitative phytochemical and acute toxicity test on the extract. African Journal of Traditional, Complementary and Alternative Medicines 2009; 6(3).
- Grover JK, Yadav S and Vats V: Medicinal plants of India with anti-diabetic potential. Journal of Ethnopharmacology 2002; 81(1): 81-10.
How to cite this article:
Kumar A, Hrathaur and Mukhopadhyay S: Unvelling the anti-diabetic efficacy of a traditional herb paradigm shift in diabetic management. Int J Pharmacognosy 2024; 11(4): 168-76. doi link: http://dx.doi.org/10.13040/IJPSR.0975-8232.IJP.11(4).168-76.
This Journal licensed under a Creative Commons Attribution-Non-commercial-Share Alike 3.0 Unported License.
Article Information
5
168-176
5406 KB
724
English
IJP
A. Kumar, Hrathaur * and S. Mukhopadhyay
College of Pharmacy, Shivalik Campus, Sihniwala, Shimla Bypass Road, Dehradun, Uttarakhand, India.
himanshi.rathaur@copdoon.org
16 April 2024
26 April 2024
27 April 2024
10.13040/IJPSR.0975-8232.IJP.11(4).168-76
30 April 2024