


NATURAL REMEDIES FOR MENOPAUSE SYMPTOMS: A REVIEW
HTML Full TextNATURAL REMEDIES FOR MENOPAUSE SYMPTOMS: A REVIEW
Yash Bhalani, Disha Prajapati * and Tanvi Dodiya
Parul Institute of Pharmacy & Research, Parul University, Limda, Tal. Waghodia, Vadodara, Gujarat, India.
ABSTRACT: Menopause is the time that marks the end of female’s menstrual cycle. It is diagnosed after a female goes 12 months without a menstrual period. It is a natural biological process divided into three phases: perimenopause, menopause and post-menopause. Menopause is associated with hormones like the Luteinizing hormone and follicle stimulating hormone various physical symptoms such as hot flashes, disruption in sleep, lower energy, osteoporosis and poor emotional health. The present study aimed to compile the treatment options available for postmenopausal symptoms, including lifestyle modifications, hormonal therapy, allopathic drugs, and herbal treatment. Various texts and online search engines like J-gate, google scholar, PUBMED, NIH, and AYUSH portals were used for the collection of data of various published research work related to menopause syndrome. Various online and offline available resources were collected, and comprehensive review was compiled considering the various aspects related to menopause symptom and available natural remedies thereof. Menopause syndrome causes debility, fragile bones, excessive bleeding, hot flushes, night sweats, burning sensations, anemia, Insomnia and mood swings. Various herbal treatment options available for the post menopause syndrome include Shatavari, Amla, Yastimadhu and Ashwagandha for debility. Pushyangachurna and Chadraprabhavati for excessive bleeding, Pravalapisti and Mukatpisti for hot flashes, Brahmi vati for mood swings and Lkashaditaila for fragile bones.
Keywords: Menopause, Natural remedies, Herbal treatment, Herbal formulation
INTRODUCTION: Menopause is the permanent cessation of menstruation due to loss of ovarian follicular function in aging women. Clinically, menopause is diagnosed after 12 months of amenorrhea, so the time of the final menses is determined retrospectively. The average age of menopause is about 51 years 1. The biological mechanism of menopause is because of changes in the function and structure of the ovaries. In the women before menopause the presence of follicles is 10 times higher than compared to after menopause.
No follicles are present in the ovaries of the postmenopausal women. This indicates that the presence of follicles in women is a determinant factor in the menopausal transition period 2. As menopause nears, the ovaries cease the formation of estrogen. When the estrogen level decreases in the body, the menstrual cycle starts to change. It can become irregular with time and then stop. The body can also adapt to some physical changes due to differences in the level of hormones like estrogen and progesterone.
The symptoms experienced during each stage of menopause are all part of body’s adjustment to these changes. Mainly menopause is divided into three stages perimenopause, menopause, and post-menopause 3.
Perimenopause: Perimenopause can begin eight to ten years before menopause; at that time, the ovaries produce less estrogen. It usually starts when women are at their forties but can start in their 30s as well. Perimenopause lasts up until menopause; it is a period when the ovarian change their function and stop releasing eggs. In the last one or two years of perimenopause, the drop in estrogen accelerates. At this time, many women may face different menopause symptoms. Women are still having menstrual cycles during this period and can get pregnant 1, 3.
Menopause: It is the permanent cessation of menstruation, a point when a woman no longer has menstrual periods. At this stage the ovaries have stopped releasing eggs and producing most of their estrogen. Menopause is diagnosed when a woman has gone without a menstrual period for twelve consecutive months 3.
Post-Menopause: Post-menopause is the period when a woman has not bleed for an entire year. During this stage, women face menopausal symptoms like hot flashes, breast cancer, and urinary tract infection. However, some women continue to experience menopausal symptoms for a decade or after a longer period of time because of the lower level of estrogen and progesterone; postmenopausal women are at increased risk for a number of health conditions like osteoporosis and heart disease. To treat this medication, hormone therapy, and healthy lifestyle changes that may reduce the risk of some of these conditions 3, 4.
Signs and Symptoms: Menopause is the final menstrual period. It starts after perimenopause in that menopause condition changes in vaginal bleeding patterns and vasomotor symptoms characterize the menopause transition. Common symptoms include vasomotor symptoms (hot flushes and night sweat), genital symptoms (vaginal dryness, dyspareunia), which may be accompanied by mood and sleep disturbance. Physical and Physiological symptoms like fragile bones (osteoporosis), excessive bleeding, anemia, urinary incontinence, reduced sexual function and depression may occur 1, 4.
Pathophysiology: The endocrinology of the menopausal transition is complex and varies considerably from woman to woman. Decreased ovarian follicles or ovulation is the basis for reproductive aging and occurs throughout life. Interactive feedback between the ovary and the hypothalamic-pituitary axis remains a challenge to understanding the endocrinology of reproductive aging. Hypothalamus produces gonadotropic releasing hormone, which stimulates the anti-pituitary to produce gonadotrophins such as Follicle Stimulating Hormone (FSH) and Luteinizing Hormone (LH) which have a major role in the ovarian cycle. FSH acts on primary follicles of the ovary and stimulates their development after passing through various stages; the follicles reach to final stages to form graphian follicles. With the help of LH graphian follicles ovulates & the ovum is released; the remaining graphian follicle forms corpus luteum. Corpus luteum produces estrogen and progesterone; these hormones prepare the uterus's endometrium for zygote implantation if there has been any fertilization.
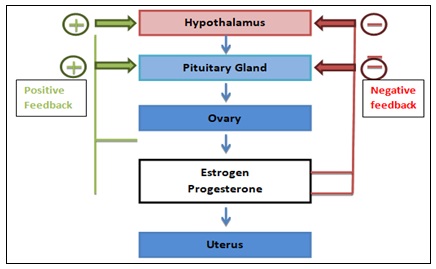
FIG. 1: PATHOPHYSIOLOGY OF MENOPAUSE
If fertilization had not occurred, then the corpus luteum slowly degenerated; hence, the estrogen and progesterone levels also fell. This leads to seeding out from the endometrium that’s called menstruation. Estrogen also provides negative feedback to the hypothalamus; hence, the FSH and LH production is lower.
During the period of menopause, there is no effective folliculogenesis, or follicle are unable to develop, so there is no ovulation or corpus luteum does not form, hence the ovary cannot secrete estrogen and progesterone hormone.
So, the endometrium does not increase, so menstruation does not occur. As the estrogen level falls, negative feedback to the hypothalamus is also abolished, so the level of FSH during menopause increases. Due to a higher level of FSH the remaining active follicles become resistant to it; hence follicles are desensitized to FSH & no folliculogenesis occurs, which leads to amenorrhea 5.
Treatment: Menopause condition is associated with difficult symptoms like hot flashes, Insomnia, fragile bones, depression, sexual dysfunction, increasing weight and decreasing in cognitive functioning. There are many treatments available for it like.
Hormonal Therapy: To overcome the deficiency of estrogen and progesterone.
Oral Administration of Estrogen: That lead to hormone concentrations in hepatic sinusoidal blood that are 4 to 5 times higher than those in peripheral blood 6.
Estrogen by Parenterally: Estrogen is administered parenterally by avoiding the first pass of metabolism in the liver. Estradiol applied to the skin by transdermal patches containing the hormone in an alcoholic solution is absorbed into the circulation at a steady rate for 3 to 4 days 7.
Combined Estrogen and Progestogen: Due to the increased risk of endometrial hyperplasia and carcinoma with the application of estrogen alone, most women who have not undergone hysterectomy are treated with a progestogen in addition to estrogen 8.
Body and Mind Interventions for Menopause Symptoms:
Hypnosis: It is a mind and body therapy that involves an extremely relaxed state of focused attention, reduced peripheral awareness, individualized mental imagery, and an enhanced capacity to respond to suggestions has been investigated for managing menopausal symptoms.
Behavioral Therapy: It is an action-oriented psychological intervention that aims to improve mental health and has been used to treat depression, hot flashes, and other menopausal symptoms.
Yoga: It is a practice that generally involves physical poses or movement sequences, conscious regulation of breathing, and mindfulness techniques that are aimed at controlling and stilling the mind, and recognizing the detached ‘witness-consciousness’ as untouched by the activities of the mind and mundane suffering and increasing the awareness or positivity.
Aromatherapy: It is also called the essential oil therapy that uses naturally extracted aromatic essences from various parts of plants, and it’s used to treat various physiological and psychological imbalances. The scented oils are believed to reduce anxiety and relax the body which may be beneficial to treating depression and mood swings in menopausal condition 9.
Alternative Medicine Approaches:
Reflexology: It is a specific type of massage where applying pressure to specific points on the feet and hands is believed to stimulate corresponding glands and organs. It is also known as zone therapy.
The principle behind this therapy is that reflex points on the hands and feet correspond to certain body zones and when pressure is applied to these parts, disease-causing energy blockages are removed from the corresponding body zone.
Homeopathy: It is a medical system based on the belief that the body can cure itself. In this treatment, patients are given dilution of natural substances that would be unfavorable to a person in ideal health condition. Some commonly used preparation includes sepia, lachesis, and pulsatilla.
Individualized formulas are prepared to treat presenting symptoms.
Acupuncture: It is a component of traditional Chinese medicine and involves inserting thin needles into the skin at certain points on the body, called acupoints. Acupuncture relieves low back pain or manages chronic pain from osteoarthritis, headaches, or neck problems 9.
Herbal Formulation: This menopausal syndrome is treated according to the various symptoms arising from the disease.
TABLE 1: LIST OF HERBAL FORMULATIONS USED IN MENOPAUSAL SYNDROME
| Class | Formulation | Use |
| Excessive Bleeding | PushyanugaChurna(10,11) | Treatment of Excessive bleeding during menstruation, estrogen imbalance in the body |
| Chandraprabhavati(12) | Treatment of Urinary infection, pain in joints and muscles and provide strength | |
| Lodhrasava syrup (13,14) | Use in craps, painful menstruation, urinary tract infection, anemia, obesity, constipation and all skin diseases | |
| Ashokarishta(15,16) | Use in heavy menstrual bleeding, pain during menstruation and menopausal symptoms | |
| DadimadiGhrita(17) | Use during menstrual bleeding, during pregnancy and to treat infertility | |
| SaptasaramKashayam(18) | Treatment of menstrual pain, painful periods, hip pain, lower back pain, constipation and low digestion power | |
| Hot flushes
|
PravalPishti(16) | Remedies for fever, gastrointestinal disorder and boosting immunity |
| Mukta Pishti(13) | Treatment of osteoporosis, prevention of anxiety and depression, regulation ofcardiac function and blood pressure | |
| Chandanasava(19) | Urinary disorders, kidney disease, leukocytospermia, and gonorrhea | |
| Kamadudha Rasa (20) | Use in chronic fever, debility after fever or chronic disease, burning sensation, vertigo, nausea and vomiting | |
| Ushirasava(21) | Heavy menstrual bleeding, night fall, bleeding disorder like rectal bleeding and nasal bleeding, anemia, skin and urinary disease | |
| DhanwantharamThailam(21) | Relief from stress, anxiety and pain, hormone regulation, and rheumatoid and osteoarthritis. | |
| Aswagandharishta(16,22,23) | Used in anemia, irregular menstruation, anxiety and improve fertility levels. | |
| ShatavariGuda(24) | Use in polycystic ovarian syndrome (PCOS) and counter the problem of menstrual pain, irregular menstrual cycle, heavy menstrual bleeding | |
| Laghu Malini Vasant rasa (25) | Used in bleeding disorders, fever, leucorrhea and disorder during pregnancy | |
| Insomnia/ Mood Swing | MansamitraVatakam(26,27) | Insomnia, schizophrenia, paranoia, panic attack and manic depressive psychosis |
| Brahmi vati(28) | Used in sleep disorder and Insomnia | |
| Brahma Rasayana(29,30) | Improve digestion and memory, retards aging and tumor growth, beats stress, exhaustion and build endurance, and bolsters immune system. | |
| Fragile bones | Lakshaditailam(31) | Useful to promote bone, muscle and muscle strength and relieve muscle and joint pain |
| Cissusequandragularis(32,33) | Joint pain, menstrual cramps, metabolic syndrome and osteoporosis | |
| Shatavari and Kukkutandatwak Bhasma (34) | Osteoporosis, decrease in bone loss and increasing the bone formation. |
Plant: Here is the list of plants whose clinical trial has been conducted for showing proper effect on the menopausal syndrome.
Valerian Root: Valerian officinalis is a perennial flowering plant native to Europe and Asian region belonging to the family of Caprifoliaceae. The double-blind clinical trial was carried by Mirabi et al., 2013 to study the effect of valerian root on Hot Flashes in menopausal women. A study was performed on 68 menopausal women with the chief complaint of hot flashes. The women in the drug group were prescribed 255 mg valerian capsule 3 times a day for 8 weeks. The women in the placebo group were prescribed identical capsules filled with starch. The results indicate that the valerian has a reduction of the hot flush frequencies 4 and 8 weeks after the treatment, so it can be considered a treatment of choice for reducing hot flashes among women who are reluctant to receive hormonal therapy due to fear or any other reason 35.
Fennel, Chamomile and Saffron: Foeniculum vulgare is a flowering plant belonging to the family of Apiaceae. Chamomile is the common name for several daisies like plant of the family Asteraceae and Saffron is a spice derived from the flower of Crocus sativus, commonly known as the “saffron crocus” belonging to the family of Iridaceae. Mahdavian et al., 2019 performed a randomized controlled clinical trial to check the effect of the mixed herbal medicine prepared from fennel seed extract, chamomile flower, and saffron stigma on menopause syndrome. A randomized, triple-blind, and placebo-controlled study was performed on 120 premenopausal women aged 45-65 years for twelve weeks. All participants took herbal extract drop orally daily and were randomly allocated in to the total four groups: Group A (250 mg chamomile, 30 mg fennel, 15 mg saffron), Group B (1000 mg, 120 mg, 60 mg), Group D (500 mg, 60 mg, 30 mg) and Group C placebo. The study evaluates 11 symptoms related to menopause.
Results reveals that the median physical score (sweating/flush, cardiac complaints, sleeping disorders, joint and muscle complaint)significantly reduces from 8.5(4) to 2(3), in psych score (depression, irritability, anxiousness and exhaustion) reduced from 12(4) to 2(2) and in urogenital score (sexual problem, urinary complaints, vaginal dryness) reduced from 6.5(3) to 3(2) in group B. in group D physical score decreased from 12(6) to 8(4), in psychological score reduced from12 (3) to 8(4) and urogenital score reduced from 7.5 (3) to 8(3) at week 12. There was no significant difference between Group A and Group C. So the 12-week extract treatment showed significant improvement in the physical, psychological, and urogenital domains in group B 36.
Jujube: Ziziphus jujuba belonging to the family of Rhamnaceaecommonly called as red date, Chinese date, and Chinese jujube. A double-blind, randomized clinical trial was performed by Mahmoudi et al., 2020. He investigated the jujube seed capsule's effect on postmenopausal women's sleep quality. The study was conducted on 106 postmenopausal women in the Khuzestan province, southwest of Iran. They divided into two groups: one intervention and the other is the control group. The intervention group received total 250 mg oral jujube seed capsule and the control group received a placebo capsule twice a day for 21 days. After the treatment, Pittsburgh sleeps quality index (PSQI) was completed in both the intervention and control group. The result reveled that after treatment the means score of sleep quality decreased in the intervention and controlled group. Although this difference was statistically significant in both intervention and control group, more reduction is observed in controlled group. And the consumption of the jujube seed capsule had a good impact on improving the sleep quality of postmenopausal women and could be recommended as a useful herbal medication 37.
Black Cohosh: A Randomized clinical trial has been performed by Shahnazi et al., 2013 to check the effect of Black Cohosh (Actaea racemose belonging to the family of Ranunculaceae) on vasomotor symptoms in postmenopausal women. The clinical trial was performed on 84 postmenopausal women. The participants were randomly divided into the two group intervention group and the control group. The intervention group received one black cohosh tablet daily, and the controlled group received one placebo tablet daily for 8 weeks. The severity of vasomotor symptoms and number of hot flashes were recorded during the pre-intervention phase and four and eight weeks after the intervention. The Experiment says there was a significant difference between the two groups in terms of severity and number of hot flashes in weeks 4 and 8 by controlling the intensity of vasomotor symptoms and the number of hot flashes before the intervention. According to the study, black cohosh seems to be an effective alternative medicine in relieving menopausal vasomotor symptoms 38.
Nigella sativa: Nigella sativa is also known as black caraway, black cumin, nigella or kalonji. It belongs to the family Ranunculaceae. A clinical trial was performed by Ibrahim et al., 2014 to see the protective effect of Nigella sativa on metabolic syndrome in menopausal women. A study was carried out on menopausal women within the age limit of 45-60 were participated and were randomly allocated into two experimental groups. Treatment group and control group. Orally administration of nigella sativa seed powder in the form of a capsule to the treatment group; a dose of 1 g per day after breakfast for the period of two months and compared to the control group given a placebo.
Anthropometric and biochemical parameters were measured at baseline, 1st month, 2nd month and a month after the treatment to determine their body weight, serum lipid profile, and fasting blood glucose (FBG). In the treatment group, there was a slight reduction with no significant difference in the body weight changes of the respondents. No significant improvement was observed in total cholesterol and blood glucose. The result revealed that the treatment with nigella sativa exerts a protective effect by improving lipid profile and blood glucose level, which are at higher risk of elevated during the menopausal period 39.
Wild yam: Dioscorea villosa belonging to the family Dioscoreaceae, is a twining tuberous vine native to eastern North America. It is commonly called as colic root, rheumatism root, devil’s bones and four-leaf yam. The clinical trial was done by Komesaroff et al., 2001 to check the effects of wild yam extract on menopausal symptoms, lipids and sex hormones in health menopausal women.
For the study double bind, placebo-controlled, cross-over study of the effect of wild yam cream was performed on 23 health women suffering from symptoms of menopause.
After a 4 week baseline period, each woman was given active cream and matching placebo for 3 months in random order. At baseline, the average body mass index was 27.3 ± 0.8, cholesterol level 5.7 ± 0.2 mmol/l and follicle stimulating hormone (FSH) level 74.2 ± 5.1 IU/l; estradiol levels were undetectable in most cases. After 3 months of treatment, no significant side effects were reported with either active treatment or placebo, and there were no changes in weight, systolic or diastolic blood pressure, or levels of total serum cholesterol, triglyceride, high-density lipoprotein (HDL) cholesterol, FSH, glucose, estradiol, or serum or salivary progesterone. The study suggested that short-term treatment with topical wild yam extract in women suffering from menopausal symptoms is free of side effects but appears to have little effect on menopausal symptoms 40.
Red Ginseng: Panax ginseng belonging to the family Araliaceae 41 was studied by Kim et al., 2012 to check the effect on menopausal symptoms and cardiovascular risk factor in postmenopausal women. The randomized, placebo controlled, double-blind clinical trial was conducted on the 72 postmenopausal women between the ages of 45 and 60. The group is divided into the two-group, intervention and controlled group. Intervention group 3 gm of red ginseng was given with 60mg of ginsenosides per day and for the control group placebo drug was given for the 12 weeks. The changes in menopausal symptoms (the Kupperman index and the menopause rating scale), cardiovascular risk factors (lipid profiles, high-sensitivity C-reactive protein, and carotid intima-media thickness), and serum estradiol levels from baseline to 12 weeks were analyzed.
In the result, significant improvements in the Kupperman index and the menopausal rating scale score were observed in the RG group compared with the placebo group. The total cholesterol and low-level density lipoprotein cholesterol significantly decreased in the group receiving the red ginseng. The red ginseng group also showed a significant deceased in carotid intima-media thickness. Serum estrogen levels were not influenced by red ginseng supplement. T5he result reveals that red ginseng could be an alternative herbal dietary supplement for reliving menopausal symptoms and conferring favorable effects on markers of cardiovascular disease in postmenopausal women 42.
St. John’s Wort: Hypericum perforatum known as perforate St John’s wort is a flowering plant in the family Hypericaceae and the type species of the genus hypericum 43. Al-Akoum et al., 2009) performed a clinical trial to check the effects of Hypericum perforatum(St. John’s wort) on hot flashes and quality of life in perimenopausal women. For the study pilot double-blind, randomized clinical trial was performed on perimenopausal women aged 40 to 65 year who experienced hot flashes (three or more per day, Heart and Estrogen/Progestin Replacement Study scale) and were randomly assigned to receive ethanolic St. John’s wort extract 900 mg and placebo. To keep a daily diary during the week before randomization and during the week before the 3 months follow-up to record hot flash frequency and intensity. A hot flash score was measured and calculated. The menopause-specific quality of life questionnaire was used to assess menopausal-specific quality of life. The 74 women were randomized. After the treatment of 12 week a nonsignificant difference favoring the St. John’s wort group was observed in the daily hot flash frequency and the hot flash score. After 3 months of treatment compared with the placebo group, women in the St. John’s wort group reported significantly better menopause-specific quality of life and significantly fewer sleep problems. The result reveals that the hypericum perforatum may improve quality of life in ways important to symptomatic perimenopausal women 44.
Liquorice and Shatavari: Liquorice or licorice is the common name of Glycyrrhiza glabra belonging to the family of Fabaceae, and Asparagus racemosus is a species of asparagus common throughout India and the Himalayas belonging to the family of Asparagaceae. A clinical study on Glycyrrhiza glabra and Asparagus racemosus was performed on menopausal symptoms by Farzana et al., 2016 study was designed as a placebo-controlled randomized, single-blind study, total 60 postmenopausal women were selected between the ages of 40 to 60 year of age. Participants were divided into two groups, A and B; Group A patients were treated with 3g of powder of Glycyrrhiza glabra and Asparagus racemosus, and Group B patients were treated with 3g of roasted wheat flour twice a day in the morning and evening for the 8-week duration.
The frequency of hot flashes and night sweats was measured in 24 hours; the Hamilton anxiety scale measured anxiety, and Insomnia by PSQIDURAT scale was recorded before and after completion of treatment. The result revealed that there was a significant improvement in the subjective and objective parameters. The drug was found to be more effective than a placebo in managing postmenopausal syndrome 45.
ACKNOWLEDGEMENT: Authors are thankful to Parul Institute of Pharmacy & Research, Parul University, Vadodara, Gujarat.
CONFLICT OF INTEREST: Authors have no conflict of interest to declare.
REFERENCES:
- Greendale GA, Lee NP and Arriola ER: The menopause 1999; 353: 571–80.
- Kargozar R, Azizi H, Salari R, Medicine C, Medicine C and Medicine C: Electronic Physician (ISSN: 2008-5842). 2017; 5826–33.
- Sowers MR and Pietra MT: La. Menopause : Its Epidemiology and Potential Association with Chronic Diseases 1995; 17(2).
- Hickey M and Rebecca A: Non-hormonal treatments for menopausal symptoms 2017; 5101(11): 1–9.
- O’Neill S and Eden J: The pathophysiology of menopausal symptoms. Obstet Gynaecol Reprod Med 2017; 27(10): 303–10.
- Kuhl H: Pharmacokinetics of oestrogens and progestogens. Maturitas 1990; 12(3): 171–97.
- Powers MS, Schenkel L, Darley PE, Good WR, Balestra JC and Place VA: Pharmacokinetics and pharmacodynamics of transdermal dosage forms of 17β-estradiol: Comparison with conventional oral estrogens used for hormone replacement. Am J Obstet Gynecol 1985; 152(8): 1099–106.
- Arafat ESS, Hargrove JT, Maxson WS, Desiderio DM, Wentz AC and Andersen RN: Sedative and hypnotic effects of oral administration of micronized progesterone may be mediated through its metabolites. Am J Obstet Gynecol 1988; 159(5): 1203–9.
- Johnson A, Roberts L and Elkins G: Complementary and Alternative Medicine for Menopause 2019; 24: 1–14.
- Kaur N, Ahuja MR and Yadav S: Physico-Chemical Evaluation of Pushyanug Churna – An Ayurvedic Compound Formulation 2016; 1: 77–81.
- Review AC, Various on, of A. A Critical Review on Various Aspects of Pushyanuga 2021; 10(6): 891–8.
- Datta N, Pal M, Roy U, Mitra R and Pradhan A: World Journal of Pharmaceutical Research. Infection 2014; 13(6): 15.
- Evaluation C and Laksha OF: Clinical Evaluation of Laksha Guggulu and Mukta Shukti Pishti in the Management of Osteopenia 2015; 4(9): 1776–84.
- Acharya N, Acharya S, Shah U, Shah R and Hingorani L: A comprehensive analysis on Symplocos racemosa: Traditional uses, botany, phytochemistry and pharmacological activities. J Ethnopharmacol 2016; 181: 236–51.
- Kumar T, Larokar YK, Jain V and Kumar Larokar Y: Standardization of different marketed brands of Ashokarishta: An Ayurvedic formulation. J Sci Innov Res 2013; 2(6): 993–8.
- Modi M, Donga S and Dei L: Clinical evaluation of Ashokarishta, Ashwagandha Churna and Praval Pishti in the management of menopausal syndrome. AYU (An Int Q J Res Ayurveda) 2012; 33(4): 511.
- Arankalle PS: Effect of dadimadi ghrita in garbhini pandu (anaemia in pregnancy). J Ayurveda Holist Med 2014; 2(3): 1–10.
- Dighe D, Ratha KK, Panda P and Rao MM: International Journal of Ayurveda 2018; 6(2): 1–9.
- Chandanasava Benefits, Uses, Dosage & Side Effects - Ayur Times.
- Kamadudha Rasa - Gastritis & Hyperacidity disorders - 250mg.
- Neve VJ, Dharkar VN. Review on Ushirasava ( fermented traditional medicine of Ayurveda ).
- Baidyanath Ashwagandharishta: Buy bottle of 450 ml Liquid at best price in India | 1mg.
- Umadevi M, Rajeswari R, Rahale CS, Selvavenkadesh S, Pushpa R and Kumar KPS: Traditional and medicinal uses of Withania somnifera. Pharma Innov 2012; 1(9): 102–10.
- Shatavari Guda - Benefits, Usage, Indications and Dosage.
- Laghu Malini Vasant ras Benefits, Dosage, Ingredients, Side Effects.
- Manasamitra Vatakam Benefits, Dosage, Ingredients And Side Effects.
- Thirunavukkarasu SV, Venkataraman S, Raja S, Upadhyay L. Neuroprotective effect of Manasamitra vatakam against aluminium induced cognitive impairment and oxidative damage in the cortex and hippocampus of rat brain. Drug Chem Toxicol 2012; 35(1): 104–15.
- Mishra D and Tubaki BR: Effect of Brahmi vati and Sarpagandha Ghana vati in management of essential hypertension – A randomized, double blind, clinical study. J Ayurveda Integr Med 2019; 10(4): 269–76.
- Brahma Rasayana: Benefits, Ingredients, Method, Dosage and Side Effects.
- Chulet R and Pradhan P: A review on rasayana. Pharmacogn Rev 2009; 3(6): 229–34.
- Lakshadi Oil - Benefits, How To Use, Ingredients, Side Effects.
- Bhujade AM, Talmale S, Kumar N, Gupta G, Reddanna P, Das SK, et al. Evaluation of Cissus quadrangularis extracts as an inhibitor of COX, 5-LOX, and proinflammatory mediators. J Ethnopharmacol 2012; 141(3): 989–96.
- Bloomer RJ, Farney TM, McCarthy CG and Lee SR: Cissus quadrangularis reduces joint pain in exercise-trained men: a pilot study. Phys Sportsmed 2013; 41(3): 29–35.
- Jasmine Japee MP: A comparitive study on shatavarei and Kukutanda twak bhasma in minimizing the risk of Postmenopausal Osteoporosis. An Int Q J Res Ayruveda. 2009; 30(3): 137.
- Mirabi P and Mojab F: The effects of valerian root on hot flashes in menopausal women. International Journal of Pharmaceutical Research 2013; 12(1): 217–22.
- Mahdavian M, Mirzaii Najmabadi K, Hosseinzadeh H, Mirzaeian S, Badiee. Aval S and Esmaeeli H: Effect of the Mixed Herbal Medicines Extract (Fennel, Chamomile, and Saffron) on Menopause Syndrome: a Randomized Controlled Clinical Trial. J Caring Sci 2019; 8(3): 181–9.
- Mahmoudi R, Ansari S, Haghighizadeh MH, Maram NS and Montazeri S: Investigation the effect of jujube seed capsule on sleep quality of postmenopausal women: A double-blind randomized clinical trial. Biomed 2020; 10(4): 42–8.
- Shahnazi M, Nahaee J, Mohammad-Alizadeh-Charandabi S and Bayatipayan S: Effect of black cohosh (Cimicifuga racemosa) on vasomotor symptoms in postmenopausal women: a randomized clinical trial. J caring Sci 2013; 2(2): 105–13.
- Ibrahim RM, Hamdan NS, Ismail M, Saini SM, Rashid SNA and Latiff LA: Protective effects of Nigella sativa on metabolic syndrome in menopausal women. Adv Pharm Bull 2014; 4(1): 29–33.
- Komesaroff PA, Black CVS, Cable V and Sudhir K: Effects of wild yam extract on menopausal symptoms, lipids and sex hormones in healthy menopausal women 2001; 144–50.
- Teas Made from Ginseng, Jujubes and Omija. Pict Korea. 2000; 31.
- Kim SY, Seo SK, Choi YM, Jeon YE, Lim KJ and Cho S: Effects of red ginseng supplementation on menopausal symptoms and cardiovascular risk factors in postmenopausal women: A double-blind randomized controlled trial. Menopause 2012; 19(4): 461–6.
- BSBI List 2007. Botanical Society of Britain and Ireland;
- Al-Akoum M, Maunsell E, Verreault R, Provencher L, Otis H and Dodin S: Effects of Hypericum perforatum (St. John’s wort) on hot flashes and quality of life in perimenopausal women: A randomized pilot trial. Menopause 2009; 16(2): 307–14.
- Samaraskera D: Inculcating Professionalism for National Development 2016.
How to cite this article:
Bhalani Y, Prajapati D and Dodiya T: Natural remedies for menopause symptoms: a review. Int J Pharmacognosy 2023; 10(7): 391-98. doi link: http://dx.doi.org/10.13040/IJPSR.0975-8232.IJP.10(7).391-98.
This Journal licensed under a Creative Commons Attribution-Non-commercial-Share Alike 3.0 Unported License.
Article Information
9
391-398
510 KB
714
English
IJP
Yash Bhalani, Disha Prajapati * and Tanvi Dodiya
Parul Institute of Pharmacy & Research, Parul University, Limda, Tal. Waghodia, Vadodara, Gujarat, India.
disha.prajapati@paruluniversity.ac.in
15 July 2023
21 July 2023
26 July 2023
10.13040/IJPSR.0975-8232.IJP.10(7).391-98
31 July 2023