


INTEGRATION OF HERBAL MEDICINES WITH CURRENT NANOTECHNOLOGY; A NEW ERA IN OBESITY MANAGEMENT IN FUTURE
HTML Full TextINTEGRATION OF HERBAL MEDICINES WITH CURRENT NANOTECHNOLOGY; A NEW ERA IN OBESITY MANAGEMENT IN FUTURE
D. M. Nirmale, Saleemulla Khan * and Chandan Pandit
Department of Pharmacognosy, P. A. College of Pharamcy, Nadupadav, Near Mangalore University, Mangalore, Karnataka, India.
ABSTRACT: Obesity and overweight is excessive or abnormal accumulation of fat in body that presents a risk to health. Overweight and obesity have reached epidemic proportions, with over four million individuals dying every year as a result of their condition. Different approaches comprising biological sources, different drug therapy, have been used in obesity treatment; though, these unoriginal selections linger unproductive and carry risks of adverse drug reaction. Hence, treatment with high efficacy and specificity is the need of the hour. Novel drug delivery system use herbal medicines and chemical entities to develop healing efficacy, target oriented through herbal approach for equilibrium, controlled release of antiobesity agents. In this review, we provide insights into current treatments for obesity with a focus on recent developments of herbal polymeric carriers for improved antiobesity drug delivery.
Keywords: Liposomes, Nanotechnology drug delivery, Herbal medicines, Anti-Obesity, Body mass index
INTRODUCTION: Obesity is a complex, chronic disease caused due to excess accumulation of adipose tissues in the body. Obesity is communal health problem evaluated in terms of fat deposition. It is the ratio between height and body mass, uneven fat distribution in human body that results in impact on health of the normal person along with financial economic burden. Obesity is confined based on 0BMI range, an individual with BMI 40 kg/m2 is severe and the one ranging in between 40–44.9 kg/m2is morbid 1. Excess fat deposition is associated with Cardiovascular, Diabetes Mellitus, Breast cancer, Asthma, Arthritis etc. BMI affects in woman’s pregnancy, chance of miscarriage, fetal abnormalities, increased risk of caesarean and delivery complications.
Prevalence of obesity is rising globally and is considered as a life-threatening health issue. The WHO, also depicted raise in epidemiological obesity rates in US 14.5% - 30.9% 2. In vice versa death risk is lower at a BMI having range at of 20–25 kg/m2. Obesity is fifth leading cause of death worldwide 3. The other parameters that indicate obesity besides raise in BP are increase in cholesterol, Triglycerides level 4. Sedentary behavior plays an important part in obesity management; according to some estimates, 30 percent of the world's population neglect to do enough exercise 4-9. Conventionally .obesity was treated with synthetic medications, which resulted in ADRs such as dry mouth, restlessness, and insomnia.
Most antiobesity medications in the Sympathomimetic category include withdrawal effects such as increased heart rate and blood pressure. Rimonabant, a cannabinoid-1 receptor antagonist, and Fenfluramine anti-obesity treatments such as sympathomimetic amines have been pulled from the market. Pancreatic lipase is a key enzyme in the absorption of fats into monoglycerides and free fatty acids and is secreted by the pancreas. The fat deposition in adipose tissue is changed when this enzyme is blocked. Due to their site specificity, binding sites, and improved specificity for drug targeting properties, various nanoparticles have been designed for obesity management use. The drug can be shielded from premature release and degradation by the herbal carrier 8, 9, 10.
Management of Obesity: Obesity is a public health problem that develops as a result of a lack of balance in nutrition, eating habits, daily routine, treatment side effects and management strategies. The importance of successful interventions cannot be overstated. Traditional therapies include a well-balanced diet, regular exercise, medication such as natural or synthetic remedies and surgical treatment such as baroctomy. When dealing with obesity, the patient should follow a balanced diet plan, make lifestyle changes, and prevent gaining energy from junk food. Beverage consumption, particularly alcohol and soft drinks, should also be avoided 11. Orlistat (Xenical), Liraglutide (Saxenda), Naltrexone (Contrave), Phentermine (Adipex-P), and Phentermine (Qsymia) are synthetic medications used to prevent fat deposition in pharmacotherapeutics and obesity management. However, commonly prescribed medications are ineffective in the treatment of obesity, and they come at an exorbitant price, and with a slew of negative side effects such as mental disorders and increased risk of heart disease 12. Supplementary studies on obesity and its cofactors such as diabetes, blood pressure, and soon have being carried out. Moving away from traditional anti-obesity medications such as herbs, medicinal plants have active constituents such as flavonoids, polyphenols, and alkaloids constituents in their management to reduce significant ADRs when compared to currently available manufactured drugs.
Conventional Obesity Treatments: Diet treatments, which include a decrease in energy intake and increase in energy expenditure to reduce obesity, have been a major focus of this research over the past decade.
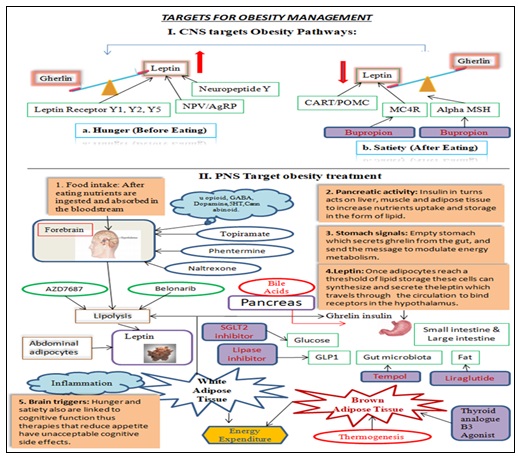
FIG. 1: OVERVIEW OF CONVENTIONAL TREATMENT APPROACHES FOR OBESITY MANAGEMENT
In today's world, investigators, experts, dieticians, doctors, and surgeons place a premium on study into the most effective weight reduction diets, such as the low-fat diet, reasonable fat diet, low carbohydrate diet, high protein diet, or extremely low-calorie diets 13. Obesity treatment relies heavily on patient compliance when it comes to food. Following that, the primary goal of obesity therapy is to provide the proper food in order to enhance the compliance level of patients with higher BMI levels, both women and men. One of the most important aspects of obesity management is to eat healthier foods and engage in regular physical activity. This reduces the risk of long-term weight gain 14, 15.
Pharmacotherapy for Obesity: The BMI range and severity of obesity or type of obesity were used to determine which drugs were administered as an additive therapy. The BMI range is 30 Kg2 to 27 Kg2. Obese people who are overweight are advised to reduce their food intake and increase their daily activity. Obesity-causing medications; the list of medicines that raise BMI is mentioned in the table, that includes few drug which are used for antiobesity treatment 16. Table 1 USFDA approved drugs such as Belviq (Lorcaserine), Aminorex, PPA are based on the mechanism of preventive hunger through reducing the level of neurotransmitters like 5HT, norepinephrine, dopaminergic drugs, withdrawn from market due to contrary effects psychiatric illnesses MI. Table 2 Weight control drugs like orlistat, an inhibitor of gastric, pancreatic lipase which impede the nutritional fat absorption 31. In light of herbal medicine's widespread acceptance for obesity therapy, owing mostly to lower ADR, an increase in public demand for a herbal carrier strategy to obesity treatment, as described in Table 3 17, 18.
TABLE 1: COMMONLY USED MEDICATIONS FOR THE TREATMENT OF OBESITY WITH THEIR DOSES AND MAJOR SIDE EFFECTS
| S. no. | Name | Dose | Side effects |
| 1 | Phentermine | 3.75/23 mg,15/92 mg once daily | Dizziness, Parasthesia, Rise in blood pressure |
| 2 | Lorcaserin | 10 mg twice daily | Headache, Nausea, Vomiting |
| 3 | Naltrexone | 32 mg/360 mg 2 tablets, Four times daily | Nausea, Vomiting, Headache, |
| 4 | Liraglutide | 3.0 mg injection once daily | Nausea, Vomiting, Pancreatitis |
| 5 | Bupropion | 32 mg/360 mg 2 tablets | Vomiting, Headache, Nausea, Dizziness, Rise in blood pressure |
TABLE 2: DRUG CLASSES ASSOCIATED WITH WEIGHT GAIN/DRUG-INDUCED OBESITY, THEIR DOSES AND SIDE EFFECTS
| S. no. | Medicines induce Obesity | Dose | Side effects |
| 1 | Antipsychotics e.g. Clozapine, Olanzapine | 25 mg - 50 mg/day, Higher dose: 900 mg/day | Nausea, vomiting, |
| 2 | Antidepressants e.g. Tricyclic antidepressant | 75 - 100 mg/day,
more than 100 mg/day |
Dry mouth, Blurred vision, Dizziness or light-headedness, Drowsiness, Restlessness |
| 3 | Antimanics e.g. Lithium | 600 mg oral 2 - 3 times/day,
900 mg oral 2 times/day, 600 mg oral 2 times/day |
Confusion, Loss of memory, fainting, fast or irregular heartbeat or pulse |
| 4 | Anticonvulsants e.g. Valproate, Gabapentin | 10-15mg/ kg/day oral route,
Doses more than 250 mg/day, 5 - 10 mg/kg/week |
Bleeding gums, Swelling of the arms, hands, feet, Cough, confusion |
| 5 | Antimigraine and Antihistaminergic drugs e.g. Cyproheptadine, flunarizine, Pizotifen | 4 mg - 20 mg/day in children | Drowsiness tired, Sleep problems,
spinning sensation |
| 6 | Antidiabetic agent’s e.g. Glitazones, insulin | 15 mg/ day, 45 mg oral/day, 45 mg oral/day. | Allergic reaction, Difficult breathing,
symptoms of liver damage |
| 7 | Glucocorticoids e.g. Dexamethasone | 5 - 60 mg orally/day | Swelling, Increase bodyweight, feeling Shortness of breath, Depression |
| 8 | Beta adrenergic receptor blocker e.g. Propranolol, Atenolol. | 0.6 mg/kg orally 2 times/ day | Depression, Confusion, Liver problems |
| 9 | Sex hormones e.g. Estrogen, Tamoxifen | 3 mg three times per day for adults, 30 – 20 mg injected into a muscle every 4 weeks as per need. | Fever, Skin inflammation,
Pain in joints and itching |
| 10 | Others e.g. Anti-neoplastic agents. | 5mg/ml in injectable solution form, 20 mg powder for the injection | Nausea, Vomiting,
Arrhythmias, Alopecia |
TABLE 3: ANTI-OBESITY AGENTS UNDER PHASE II AND PHASE III CLINICAL TRIALS
| S. no. | Medicines in phase II trials | Medicines in phase III trials |
| 1 | Dopaminergic inhibitore.g. Bupropion | Adrenergic agonist e.g. Mazindol |
| 2 | CCK A antagonist e.g. Linitript | SSRT inhibitor e.g. Sertraline |
| 3 | Pegylated leptin | TRH analogue e.g. Posatirelin |
| 4 | DPP IV inhibitors | Cannabinoid antagonists |
| 5 | Human growth hormone e.g.AOD9604 | Lipase inhibitor, ATL-962 |
| 6 | Phytostanol | Lipase inhibitor |
Advance Clinical Treatment Aspects: Despite progress over the last two decades, traditional obesity therapy approaches are frequently insufficient for protecting ME and avoiding life-threatening ADRs. Surgical techniques include GIT bypass, gastrectomy, adaptive gastric band, biliopancreatic diversion, and duodenal switch 19. Surgical procedures are simple to do for patients with weight gain who are not responding to drug therapy and a diet regimen has been shown to be useful in the treatment of obesity 20.
Confines over Traditional Antiobesity Treatment: Obesity treatment options are limited due to adverse drug reactions (ADR). When consumers choose for a conservative treatment, they are usually disappointed. Despite the diet therapy, the most significant drawback of the obese patient's is sporadic adherence to the diet, which results in erratic results, implying dissatisfaction with the therapy. Hypertension, dyslipidemia increased risk of mental ADRs including Depression, Anxiety, Stroke, and nonfatal myocardial infraction are all risk factors associated with obesity treatment. The most common adverse reaction to the medications sibutramine and orlistat is an increase in heart rate and blood pressure. These ADRs of conventional obesity management play an important role in changing social views to natural remedies for obesity management 21, 22.
Herbal Nanotechnology for Obesity Treatment: Herbal nanotechnology has had an impact on the development of innovative NDDS. Sizes of vesicles range from 10 to 100 nm. The novels are concerned with increasing drug bioavailability in order to increase drug interest. This nanocarrier plays a critical role in nanotherapeutics, which are derived from herbs such as apigenin, revesetrol, piperine, and capsaicin. At the nanoscale level, the surface area of the nanocarrier increases, allowing for the loading of nanoparticles at therapeutic and diagnostic levels for the treatment of obesity.
This herbal nanotechnology based on a new method has explored to increase bioavailability result in improved cell uptake, controlled release, improved solubility, therapeutic drug target, reduced dose, enhancement in pharmacological action compared to the free herbal drugs. Nano therapy which helps in treatment of Cancer, Dibetes, Obesity, Viral infection, long term hormonal therapy means in case assisted reproductive procedures. Henceforth integration of herbal medicines with current nanotechnology opens a new era in obesity therapeutics in upcoming future 70, 71, 73, 74.
Nanocarrier for the Targeted Drug Delivery System: Obesity has been treated with herbal nanocarriers such as Reseversetrol, Capsicin, and hydrocitric acid. These medications have been combined in obesity control using various nanocarriers such as liposomes, micelles, polymeric nanoparticles, gold, silver, PEG, Dendrimers, and SLN integrated biomolecules at specified sites Table 4, 5 and 6 75, 76, 79, 80, 100.
TABLE 4: NANOCARRIERS EMPLOYED IN DRUG DELIVERY SYSTEMS FOR OBESITY MANAGEMENT
| S. no. | Carrier matrix (Nanocarrier) | Experimental model | Reference |
| 1 | PLGA | Mice fed HFD, Normal diet | 90,98 |
| 2 | Methylcellulose-gold nanoparticle | 3T3-L1 cells. | 91,98 |
| 3 | Hydrocitric acid | HFD induced obese mice | 92,98 |
| 4 | PCL | Obese rats induced by hypothalamic lesion using monosodium L-glutamate | 93,98 |
| 5 | Chitosan | HFD-induced obese rats | 94,98 |
| 6 | Cerium oxide | Lean rats | 95,98 |
| 7 | Gold | Mice fed HFD or normal diet | 96,98 |
| 8 | Linseed oil | HFD-induced obese mice | 97,98 |
TABLE 5: MEDICINAL PLANTS REPORTED TO POSSESS ANTI-OBESITY POTENTIAL
| S. no. | Plant name | Family | Parts used | Reference |
| 1 | Achyranthes aspera Linn | Amaranthaceae | Seed | 29 |
| 2 | Acorus calamus Linn | Araceae | Roots and leaves | 30 |
| 3 | Achyranthesbidentata Blume | Amaranthaceae | Root | 31 |
| 4 | Actinidia polygama Max | Actinidiaceae | Fruits | 32 |
| 5 | Ade nophora triphylla Hara | Campanulaceae | Root | 33 |
| 6 | Aegle marmelos Linn | Rutaceae | Leaves | 34 |
| 7 | Allium cepa Linn | Amaryllidaceae | Peel | 35 |
| 8 | Allium fistulosum Linn | Liliaceae | Root | 36 |
| 9 | Allium nigrum Linn | Amaryllidaceae | Bulb | 37 |
| 10 | Allium sativum Linn | Amaryllidaceae | Stem, Bulb and Root | 38 |
| 11 | Alpinia galanga Linn | Zingiberaceae | Rhizome | 39 |
| 12 | Alpinia officinarum Hance | Root | 40 | |
| 13 | Angelica gigas Naka | Apiaceae | Roots | 41 |
| 14 | Argyreia nervosa Bojer | Convolvulaceae | Root | 42 |
| 15 | Artemisia iwayomogi | Compositae | Whole Plant | 43 |
| 16 | Atractylodes lancea | Compositae | Rhizome | 44 |
| 17 | Aster pseudoglehni Lim | Asteraceae | Leaves | 45 |
| 18 | Bauhinia variegate Linn | Leguminosae | Stem, root Barks | 46 |
| 19 | Bergenia crassifolia (L.) Fritsch | Saxifragaceae | Leaf | 47 |
| 20 | Boehmeria nivea (L.) Gaudich | Urticaceae | Leaf | 48 |
| 21 | Bombax ceiba L. | Malvaceae | Stem bark | 49 |
| 22 | Anredera cordifolia | Basellaceae | Leaves | 50 |
| 23 | Brassica rapa L | Brassicaceae | Root | 51 |
| 24 | Buddleja officinalis | Scrophulariaceae | Whole Plant | 52 |
| 25 | Bursera grandiflora | Burseraceae | Roots | 53 |
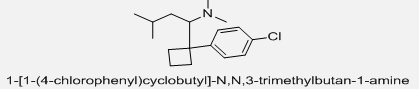
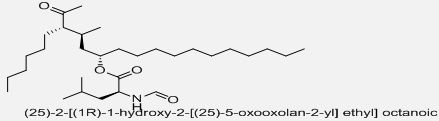
TABLE 6: CHEMICAL STRUCTURES OF SELECTED SYNTHETIC ANTI-OBESITY DRUGS AND BIOACTIVE PHYTOCONSTITUENTS WITH ANTI-OBESITY POTENTIAL
| Sibutramine
|
 |
| Orlistat
|
 |
| Rimonabant | 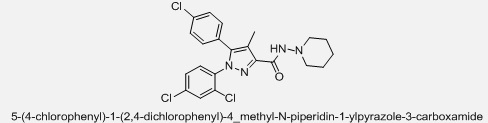 |
| Lorcaserine |  |
| Phendimetrazine
|
 |
| Diethylpropion
|
 |
| Methamphetamine
|
 |
| Phentermine
|
 |
| Topiramate |  |
| Caffeine
|
 |
| Theophylline
|
 |
| Theobromine
|
 |
| Fucoxanthinol
|
 |
| Rutin
|
 |
| Kaempferol
|
 |
| Quercetin |  |
| Luteolin
|
 |
| Catechin
|
 |
| (-)-epigallocatechin
|
 |
| Theaflavin
|
 |
| Chlorogenic acid
|
 |
| Sessiloside
|
 |
| Copteroside B
|
 |
| Dioscin
|
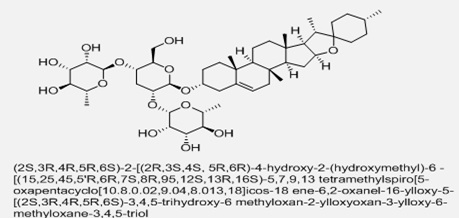 |
| Gracillin
|
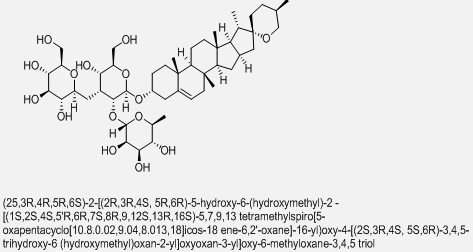 |
| Crocin
|
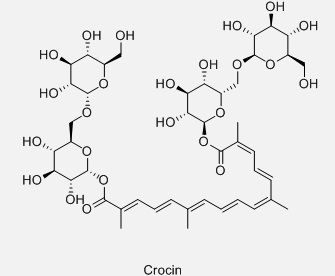 |
| Asiatic acid
|
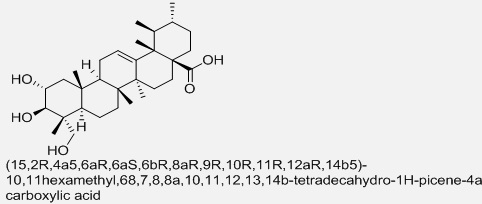 |
| Betulinic acid |  |
| Carnosic acid
|
 |
| Carnosol
|
 |
| Oleanolic acid
|
 |
| Valilactone
|
 |
| Vibralactone
|
 |
| Esterastin
|
 |
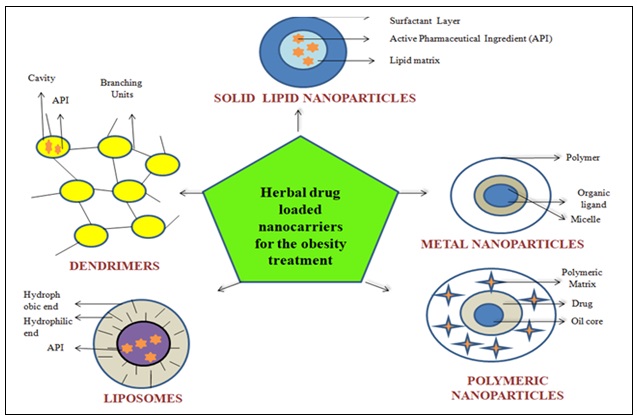
FIG. 2: SCHEMATIC REPRESENTATION OF HERBAL NANOTECHNOLOGY-BASED DRUG DELIVERY SYSTEMS FOR OBESITY MANAGEMENT
Liposomes: A concentric membrane lipid layer with a hydrophilic head on one end and a hydrophobic tail on the other end compensates nanoparticles. In the water phase, HN is integrated into lipids. Combining herbal carriers such as apigenin, reservetrol, and HA with liposomes as carriers for herbal medicine enhances the active components' stability, acceptability, and toxicity 81, 82. Dr. Prof. Alec D. Bangham, a British haematologist, created the word liposome. Liposomes are spherical in shape and contain a double layer of water on the interior or outside. Because of their limited solubility in the aqueous phase, lipophilic and hydrophilic medicines are locked inside the double layer. Furthermore, due to RES, the edges of this two-layer DDS were swiftly eliminated from the body. The opsonin proteins, which act as a receptor on membranes with a diameter of 50–200 nm, are ejected from the bloodstream into the spaces between irregular cells in the tissue. Nanoparticles are nano-sized particles created by combining PEG molecules. PEG, PLGA, and PCL are carriers that aid in the efficient uptake of herbal drugs in the treatment of obesity 77, 78, 89.
Micelles: This technique entraps herbal drug micelles and is spherical nanosized in nature, with a hydrophobic drug at the core and a hydrophobic zone linked to the surrounding solvent 85, 86. If you're looking for a unique way to express yourself Polymer micelles, which are widely used for hydrophobic drugs, were developed to increase RES, permeability, retention time, and to entrap various types of remedies in the inner core. PEG-2500 and PCL -1200 were used to create multifunctional block copolymer micelles. Micelles were absorbed and delivered to the nuclei of EGFR-positive BC cells in a substantial way. DDS appears to be a good treatment option for BC 89.
Solid Lipid Nanoparticles (SLN): SLN is a lipid monolayer that is nontoxic and stable and it has a hard lipid core that is employed in the DDS. It's simple to scale up production with particle sizes ranging from 50 to 1000 nm. SLN combines the herbs' low-water-soluble elements to improve absorption, stability, and reduce negative effects at the targeted site, as well as provide a longer-lasting benefit in the treatment of obesity 83, 84.
In the adriamycin-resistant HBC MCF-7 cell line, doxorubicin loaded polymeric micelles showed improved loading, prolonged release, and substantial accelerated uptake 89.
Dendrimers: This is a branched, core macromolecule with a branching structure that enables for conjugation at a specific point and is used to treat obesity. These are highly branched molecules with a well-defined core, ranging in size from 1 to 15 nm. It is divided into three sections: core, branches, and surface. Dendrimers are an ideal carrier for drug delivery because of their monodispersity, water solubility, encapsulation capabilities, and huge number of functional groups. In comparison to liposomes and micelles, dendrimer-drug conjugates are more stable, easy to synthesise, and sterilize because to their unimolecular structure. Dendrimers are distinguished from other drug delivery carriers such as micelles, liposomes, and emulsion droplets by their capacity to attach cell-specific targeting groups, solubility modifiers, and imaging tags to a dendritic surface in a well-controlled manner 89.
Metal Nanoparticles (MN- Gold, Copper): Metals like iron oxide and gold, which have benign, non-toxic qualities, are being investigated for their drug loading capability in this delivery method, which is used to treat obesity 87, 88.
Pb nanoparticles in the size range of 1 nm to 150 nm have exhibited single chemical and physical capabilities for transporting and unloading active components. Tamoxifen-polyethylene glycol-thiol gold nanoparticles conjugates were designed to selectively target the hormonal therapy for many types of reproductive diseases. Tamoxifen-polyethylene glycol- thiol GNconjugates developed to selectively target, GNused to target the hormonal therapy for different kind of reproductive disease.
Carbon Nanotubes (CN): These are graphitic carbon CN with exceptional properties that have developed as a new approach for transporting medicinal compounds. The CN site is involved in the transport of peptides, proteins, and AGCT. Simply solitary walled carbon nanotubes were used for site-specific drug administration because to cell membranes, which had decreased toxicity and immunogenicity 89.
CONCLUSION: In antiobesity management, various medicinal plants and their bioactive components differs, nanotherapeutics can help to see the potential of those bioactive substances as anti-obesity, anti-cancer, and hormonal therapy for overcoming drug side effects. Straight pharmacological therapy appears to improve the active components' therapeutic utility. The main drawback is treatment failure, which is largely due to the behavior of today's generation newborns, i.e., adolescents and adults who are predisposed to consume fats and sugar-containing foods in their daily lives 99.
ACKNOWLEDGEMENT: Nil
CONFLICT OF INTEREST: Nil
REFERENCES:
- Wyatt SB, Winters KP and Dubbert PM: Overweight and obesity: prevalence, consequences, and causes of a growing public health problem. Am J Med Sci 2006; 331(4): 166–174.
- Kopelman PG: Obesity as a medical problem, Nature 2000; 404(6778): 635.
- The problem of overweight and obesity, preventing and managing the global epidemic. WHO Technical Report Series 2000; 894: 5-37.
- Zimmet PZ and Alberti KG: Introduction globalization and the noncommunicable disease epidemic. Obesity 2006; 14(1): 1-3.
- Flegal KM, Carroll MD, Kuczmarski RJ and Johnson CL: Overweight and obesity in the United States. Prevalence and trends. Int J Obes Relat Metab Disord 22: 39-47.
- Ramachandran A and Snehalatha C: Rising burden of obesity in Asia. J Obes 2010; 1-8.
- John A, Vetrivel U, Sivashanmugam M and Natarajan SK: Microsecond simulation of the proteoglycan-like region of carbonic anhydrase IX and design of chemical inhibitors targeting pH homeostasis in cancer cells. ACS Omega 2020; 5(8): 4270–4281.
- Losson H, Schnekenburger M, Dicato M and Diederich M: HDAC6 - an emerging target against chronic myeloid leukemia. Cancers 2020; (2): 318.
- Singh R, Bhardwaj VK, Sharma J, Das P and Purohit R: Discovery and in-silico evaluation of aminoarylbenzosuberene molecules as novel checkpoint kinase 1 inhibitor determinants. Genomics 2020.
- Ge Y: Using Molecular Simulations and Statistical Models to Understand Bimolecular Conformational Dynamics, Temple University, ProQuest Dissertations Publishing, 2020; 27744518.
- Wu X, Sun H, Qin Z, Che P, Yi X, Yu Q, Zhang H, Sun X, Yao F and Li J: Fully physically crosslinked pectin-based hydrogel with high stretchability and toughness for biomedical application. Int J Biol Macromol 2020; 149: 707–716.
- Madadlou A, Rakhshi E and Abbaspourrad A: Engineered emulsions for obesity treatment. Trends Food Sci Technol 2016; 52: 90–97.
- Ibrahim MM: Subcutaneous and visceral adipose tissue: structural and functional differences. Obes Rev 2010; 11(1): 11–18.
- Parasuraman S and Wen LE: Animal Model for obesity –An overview. Sys Rev Pharm 2015; 6(1): 9-12.
- Wadden TA: Treatment of obesity by moderate and severe caloric restriction results of clinical research tracts. Ann Intern Med 1993; 119: 688-693.
- Ashley JM, St Jeor ST, Schrage JP, Perumean Chaney SE, Gilbertson MC, McCall NL and Bovee V: Weight control in the physician's office. Arch Intern Med 2001; 161: 1599-1604.
- Anderssen S, Holme I, Urdal P and Hjermann I: Diet and exercise intervention have favourable effects on blood pressure in hypertensives: The Oslo Diet and Exercise Study (ODES). Blood Press 1995; 4: 343-349.
- Bertram SR, Venter I and Stewart RI: Weight loss in obese women exercise versus dietary education. S Afr Med J 1990; 78: 15-18.
- Anderssen S, Holme I, Urdal P and Hjermann I: Diet and exercise intervention have favourable effects on blood pressure in hypertensives: The Oslo Diet and Exercise Study (ODES). Blood Press 1995; 4: 343-349.
- Wood PD, Stefanick ML, Dreon DM, Frey-Hewitt B, Garay SC, Williams PT, Superko HR, Fortman SP, Albers JJ and Vranizan KM: Changes in plasma lipids and lipoproteins in overweight men during weight loss through dieting as compared with exercise. N Engl J Med 1988; 319: 1173-1179.
- Ditschuneit HH, Flechtner-Mors M, Johnson TD and Adler G: Metabolic and weight loss effects of long-term dietary intervention in obese patients. Am J Clin Nutr 1999; 69: 198-204.
- US Department of Health and Human Services: Leading health indicators. Overweight and obesity. Healthy people 2010 (Conference ed. in two volumes). DC. US Department of Health and Human Services, Washington 2000; 24-45.
- Wyatt HR, Wing RR and Hill JO: The National weight control registry. In: Evaluation & Management of obesity Edited by: Bessesen DH, Kushner RF. Philadelphia, Hanley & Belfus Inc 2002; 199-224.
- Schoeller DA, Shay K and Kushner RF: How much physical activity is needed to minimize weight gain in previously obese women. Am J Clin Nutr 1997; 66: 551-556.
- Physical Activity and Health: A Report of the surgeon General PA. US Department of Health and Human Services 1996.
- National Institutes of Health (NHLBI): Clinical guidelines on the identification, evaluation and treatment of overweight and obesity in adults. The evidence reports Washington D.C. National Institute of Health, Obese Res 1998; 6: 51-201.
- Lessof MH and Myerson A: Benzedrine sulfate as an aid to be the treatment of obesity. N Engl J Med 1938; 218: 119-205.
- Connolly HM, Crary JL, McGoon MD, Hensud DD, Edwards BS and Edwards WD: Valvular heart disease associated with fenfluramine, phentermine. N Engl J Med 1997; 337: 783.
- James WP, Astrup A, Finer N, Hilsted J, Kopelman P, Rossner S, Saris WH and Van Gaal LF: Effect of sibutramine on weight maintenance after weight loss: a randomized trial. STORM Study Group. Sibutramine Trial of Obesity Reduction and Maintenance. Lancet 2000; 356: 2119-2125.
- Mun EC, Blackbur GL and Matthews JB: Current status of medical and surgical therapy for obesity. Gastroenterology 2001; 120: 669-681.
- Rolls BJ, Shide DJ, Thorwart ML and Ulbrecht JS: Sibutramine reduces food intake in non-dieting women with obesity. Obes Res 1998; 6: 1-11.
- Hansen DL, Toubro S, Stock MJ, and Macdonald IA and Astrup A: Thermogenic effects of sibutramine in humans. Am J Clin Nutr 1998; 68: 1180-1186.
- Seagle HM, Bessesen DH and Hill JO: Effects of sibutramine on resting metabolic rate and weight loss in overweight women. Obes Res 1998; 6: 115-121.
- Astrup A and Toubro S: When, for whom and how to use sibutramine.Int J Obes Relat Metab Disord 2001; 25: 52-57.
- Luque CA: Sibutramine: a serotonin-norepinephrine reuptake inhibitor for the treatment of obesity. Ann Pharmacotherapy 1999; 33: 968-978.
- Sjostrom L, Rissonen A, Andersen T, Boldrin M, Golay A and Koppeschaar HP: Randomized placebo-controlled trial of orlistat for weight loss and prevention of weight in obese patients. European Multicenter Orlistat study group. Lancet 1998; 352: 167-172.
- Rani N, Sharma SK and Vasudeva N: Assessment of Antiobesity Potential of Achyranthes aspera Seed. Evid Based Complement Alternat Med 2012; 715912.
- Mythili Avadhani MN: The Sweetness and Bitterness of Sweet Flag [Acorus calamus] – A Review. Research Journal of Pharmaceutical, Biological and Chemical Sciences 4: 598-610.
- Oh SD, Kim M, Min BI, Choi GS and Kim SK: Effect of Achyranthes bidentata Blume on 3T3-L1 Adipogenesis and Rats Fed with a High-Fat Diet. Evid Based Complement Alternat Med 2014; 158018.
- Sung YY, Yoon T, Yang WK, Moon BC, Kim HK Antiobesity effects of Actinidia polygama extract in mice with high fat diet induced obesity. Mol Med Rep 2013; 7: 396-400.
- Hyun-Jin C, Mi Ja C and Seung-Shi H: Antiobese and hypocholesterolaemic effects of an Adenophora triphylla extract in HepG2 cells and high fat diet-induced obese mice. Food Chemistry 2010; 119: 437–444.
- Lee SE, Lee EH, Lee TJ, Kim SW and Kim BH: Anti-obesity effect and action mechanism of Adenophora triphylla root ethanol extract in C57BL/6 obese mice fed a high-fat diet. Biosci Biotechnol Biochem 2013; 77: 544-550.
- Karmase A, Birari R and Bhutani KK: Evaluation of anti-obesity effect of Aegle marmelos Phytomedicine 2013; 20: 805-812.
- Karmase A, Jagtap S and Bhutani KK: Anti-adipogenic activity of Aegle marmelos Phytomedicine 2013; 20: 1267-1271.
- Kim OY, Lee SM, Do H, Moon J and Lee KH: Influence of quercetin-rich onion peel extracts on adipokine expression in the visceral adipose tissue of rats. Phytother Res 2012; 26: 432-437.
- Moon J, Do HJ, Kim OY and Shin MJ: Antiobesity effects of quercetin-rich onion peel extract on the differentiation of 3T3-L1 preadipocytes and the adipogenesis in high fat-fed rats. Food Chem Toxicol 2013; 58: 347-354.
- Sung YY, Yoon T, Kim SJ, Yang WK and Kim HK: Anti-obesity activity of Allium fistulosum extract by down-regulation of the expression of lipogenic genes in high-fat diet-induced obese mice. Mol Med Rep 2011; 4: 431-435.
- Sung YY, Yoon T, Kim SJ, Yang WK and Kim HK: Anti-obesity activity of Allium fistulosum extract by down-regulation of the expression of lipogenic genes in high-fat diet-induced obese mice. Mol Med Rea 2011; 4: 431-435.
- Chen YC: Methanolic extract of black garlic ameliorates dietinduced obesity via regulating adipogenesis, adipokine biosynthesis, and lipolysis. Journal of Functional Foods 2014; 9: 98-108.
- Kim I, Kim HR, Kim JH and Om AS: Beneficial effects of Allium sativum stem extract on lipid metabolism and antioxidant status in obese mice fed a high-fat diet. J Sci Food Agric 2013; 93: 2749-2757.
- Lai YS: Garlic essential oil protects against obesity-triggered nonalcoholic fatty liver disease through modulation of lipid metabolism and oxidative stress. J Agric Food Chem 2014; 62: 5897-5906.
- Kumar S and Alagawadi KR: Anti-obesity effects of galangin, a pancreatic lipase inhibitor in cafeteria diet fed female rats. Pharm Biol 2013; 51: 607-613.
- Jung CH, Jang SJ, Ahn J, Gwon SY and Jeon TI: Alpinia officinarum inhibits adipocyte differentiation and high-fat dietinduced obesity in mice through regulation of adipogenesis and lipogenesis. J Med Food 2012; 15: 959-967.
- Xia DZ, Yu XF, Wang HM, Ren QY and Chen BM: Anti-obesity and hypolipidemic effects of ethanolic extract from Alpinia officinarum Hance (Zingiberaceae) in rats fed high-fat diet. J Med Food 2010; 13: 785-791.
- Hwang JT: Decursin, an active compound isolated from Angelica gigas, inhibits fat accumulation, reduces adipocytokine secretion and improves glucose tolerance in mice fed a high-fat diet. Phytother Res 2012; 26: 633-638.
- Kumar S, Alagawadi KR and Rao MR: Effect of Argyreia speciosa root extract on cafeteria diet-induced obesity in rats. Indian J Pharmacol 2011; 43: 163-167.
- Choi Y, Yanagawa Y, Kim S, Whang WK and Park T: (Artemisia iwayomogi extract attenuates high-fat diet-induced obesity by decreasing the expression of genes associated with adipogenesis in mice. Evid Based Complement Alternat Med 2013; 915953.
- Jiao P, Tseng-Crank J, Corneliusen B, Yimam M and Hodges M: Lipase inhibition and antiobesity effect of Atractylodes lancea. Plant Med 2014; 80: 577-582.
- Lee HM, Yang G, Ahn TG, Kim MD and Nugroho A: Antiadipogenic effects of aster glehni extract: in-vivo and in-vitro Evid Based Complement Alternat Med 2013; 859624.
- Balamurugan G and Muralidharan P: Antiobesity effect of Bauhinia variegata bark extract on female rats fed on hypercaloric diet. Bangladesh Journal of Pharmacology 2010; 5: 8-12.
- Shikov AN, Pozharitskaya ON, Makarova MN, Makarov VG and Wagner H: Bergenia crassifolia (L.) Fritsch--pharmacology and phytochemistry. Phytomedicine 2014; 21: 1534-1542.
- Lee JJ: Effects of ramie leaves on improvement of lipid metabolism and antiobesity effect in rats fed a high fat/high cholesterol diet. Korean Journal of Food Science and Technology 2011; 43: 83-90.
- Khalid M and Siddiqui HH: Evaluation of weight reduction and anti–cholesterol activity of Punarnava root extract against high fat diets induced obesity in experimental rodent. Asian Pacific Journal of Tropical Biomedicine 2012; 2: 1323-1328.
- Gupta P, Goyal R, Chauhan Y and Sharma PL: Possible modulation of FAS and PTP-1B signaling in ameliorative potential of Bombax ceiba against high fat diet induced obesity. BMC Complement Altern Med 2013; 13: 281.
- Kim H and Choung SY: Anti-obesity effects of Boussingaulti gracilis Miers var. pseudobaselloides Bailey via activation of AMP-activated protein kinase in 3T3-L1 cells. J Med Food 2012; 15: 811-817.
- An S, Han JI, Kim MJ, Park JS and Han JM: Ethanolic extracts of Brassica campestris rapa roots prevent high-fat diet-induced obesity via beta (3)-adrenergic regulation of white adipocyte lipolytic activity. J Med Food 2010; 13: 406-414.
- Roh C, Park MK, Shin HJ, Jung U and Kim JK: Buddleja officinalis Maximowicz extract inhibits lipid accumulation on adipocyte differentiation in 3T3-L1 cells and high-fat mice. Molecules 2012; 17(2012): 8687- 8695.
- Thovhogi N: Targeted delivery using peptide-functionalized gold nanoparticles to white adipose tissues of obese rats, J. Nanoparticle Res 2015; 17(2): 112.
- Nelson B: Antioxidant cerium oxide nanoparticles in biology and medicine. Antioxidants 2016; 5(2): 15.
- Rocca A: Pilot in-vivo investigation of cerium oxide nanoparticles as a novel anti-obesity pharmaceutical formulation, Nanomed. Nanotechnology. Biol Med 2015; 11(7): 1725–1734.
- Wahajuddin SA: Superparamagnetic iron oxide nanoparticles: magnetic nanoplatforms as drug carriers, Int. J. Nanomed 2012; 7: 3445.
- Sharifi S: Superparamagnetic iron oxide nanoparticles alter expression of obesity and T2D-associated risk genes in human adipocytes. Sci Rep 2013; 3: 2173.
- Hossen MN: A comparative study between nanoparticle-targeted therapeutics and bioconjugates as obesity medication, J. Contr. Release 2013; 171(2): 104–112.
- Hossen MN: Therapeutic assessment of cytochrome C for the prevention of obesity through endothelial cell-targeted nanoparticulate system. Mol Ther 2013; 21(3): 533–541.
- Lacatusu I: Improved anti-obesity effect of herbal active and endogenous lipids co-loaded lipid nanocarriers: preparation, in-vitro and in-vivo Mater Sci Eng C 2019; 99: 12–24.
- Joo JI: Proteomic analysis for antiobesity potential of capsaicin on white adipose tissue in rats fed with a high fat diet, J. Proteome Res 2010; 9(6): 2977–2987.
- Wang S: Resveratrol induces brown-like adipocyte formation in white fat through activation of AMP-activated protein kinase (AMPK) α1. Int J Obes 2015; 39(6): 967.
- Walle T: High absorption but very low bioavailability of oral resveratrol in humans, Drug Metabol. Dispos 2004; 32(12): 1377–1382.
- Zu Y: Resveratrol liposomes and lipid nanocarriers: comparison of characteristics and inducing browning of white adipocytes, Colloids Surf. B Biointerfaces 2018; 164: 414–423.
- Takke A and Shende P: Nanotherapeutic silibinin: an insight of phytomedicine in healthcare reformation, Nanomed. Nanotechnol. Biol Med 2019; 102057.
- Ezhilarasi P, Muthukumar S and Anandharamakrishnan C: Solid lipid nanoparticle enhances bioavailability of hydroxycitric acid compared to a microparticle delivery system, RSC Adv 2016; 6(59): 53784–53793.
- El-Menshawe SF: Nanosized soy phytosome-based thermo gel as topical anti-obesity formulation: an approach for acceptable level of evidence of an effective novel herbal weight loss product. Int J Nanomed 2018; 13: 307.
- Chawla P, Kumar M and Khan H: A review on effective approach of biogenic metal nanoparticles contrary to obesity. Allergy Clin Immunol 141(4): 1169-1179.
- Lee JH and Kim JC: Effect of cubic phase nanoparticle on obesity-suppressing efficacy of herbal extracts. Biotechnol Bioproc Eng 2015; 20(6): 1005–1015.
- Razavi R, Kenari RE, Farmani J, Jahanshahi M: Fabrication of zein /alginate delivery system for nanofood model based on pumpkin. Int J Biol Macromol 2020.
- Low LE, Wong SK, Chew CL and Tang SY: Principles and potential applications of cavitation technology for nano-foods. In Nano-food Engineering, Springer Cham 2020; 125–152.
- Widakowich C, Azambuja E. de, Gil T, Cardoso F, Dinh P, Awada A and Piccart-Gebhart M: targeted therapies in breast cancer: Where are we now. The International J of Biochemistry & Cell Biology 2007; 39: 1375 – 87
- Zhang XZ: Polymeric in situ hydrogel implant of epigallocatechin gallate (EGCG) for prolonged and improved antihyperlipidemic and anti-obesity activity: preparation and characterization. J Biomater Tissue Eng 2015; 5: 813–817.
- Liao ZX: Light-triggered methylcellulose gold nanoparticle hydrogels for leptin release to inhibit fat stores in adipocytes. International Journal of Nanomedicine 2017; 12: 7603–7611.
- Jung H: Anti-obesity effect of a novel caffeine-loaded dissolving microneedle patch in high-fat diet-induced obese C57BL/6J mice. J Control Release 2017; 265: 41–47.
- Almeida MA: Enhanced gastric tolerability and improved anti-obesity effect of capsaicinoids-loaded PCL microparticles. Materials Science and Engineering C 2014; 40: 345–356.
- Tan S: Antiobese effects of capsaicin- chitosan microsphere (CCMS) in obese rats induced by high fat diet. J Agric Food Chem 2014; 62: 1866–1874.
- Rocca A: Pilot in-vivo investigation of cerium oxide nanoparticles as a novel anti-obesity pharmaceutical formulation. Nanomedicine 2015; 11: 1725–1734.
- Thovhogi N: Targeted delivery using peptide-functionalized gold nanoparticles to white adipose tissues of obese rats. J Nanoparticle Res 2015; 17: 112.
- Lacatusu I: Improved anti-obesity effect of herbal active and endogenous lipids co-loaded lipid nanocarriers: Preparation, in-vitro and in-vivo Mater Sci Eng C 2019; 99: 12–24
- Di Huang, Meng Deng and Shihuan Kuang: Trends in Endocrinology & Metabolism 2019; 30(12): 974-989.
- Dnyaneshwar Nirmale and Sunil S. Jalalpure: Insight into the interaction of human pancreatic lipase with potential anti-obesity drug. Cetilistat, using a Molecular Docking and Molecular Dynamics Simulation 2022; 10: 53388.
How to cite this article:
Nirmale DM, Khan S and Pandit C: Integration of herbal medicines with current nanotechnology; a new era in obesity management in future. Int J Pharmacognosy 2026; 13(7): 651-65. doi link: http://dx.doi.org/10.13040/IJPSR.0975-8232.IJP.13(7).651-65.
This Journal licensed under a Creative Commons Attribution-Non-commercial-Share Alike 3.0 Unported License.
Article Information
4
651-665
13095 KB
7
English
IJP
D. M. Nirmale, Saleemulla Khan * and Chandan Pandit
Department of Pharmacognosy, P. A. College of Pharamcy, Nadupadav, Near Mangalore University, Mangalore, Karnataka, India.
saleemulla.khan@gmail.com
26 May 2026
22 June 2026
29 June 2026
10.13040/IJPSR.0975-8232.IJP.13(7).651-65
01 July 2026