


DIABETES AND ANTIDIABETIC HERBAL FORMULATIONS: AN ALTERNATIVE TO ALLOPATHY
HTML Full TextDIABETES AND ANTI-DIABETIC HERBAL FORMULATIONS: AN ALTERNATIVE TO ALLOPATHY
Maninder Kaur * and Vandana Valecha
Faculty of Pharmaceutical Sciences, Doon Valley Institute of Pharmacy and Medicines, Karnal - 132001, Haryana, India.
ABSTRACT: The present study was based on diabetes, its cure & herbal products available in the market. Diabetes mellitus is the most common endocrine disorder, affecting 16 million individuals in the United States and 200 million worldwide. Despite the use of advanced synthetic drugs for the treatment, use of herbal remedies is gaining higher importance because of synthetic drugs have drawbacks and limitations. The herbal drugs with anti-diabetic activity are extensively formulated commercially because of easy availability, affordability and fewer side effects as compared to synthetic anti-diabetic drugs. Anti-diabetic herbal formulations (AHF) are considered to be more effective for the management of diabetes. There are around 600 herbal drug manufacturers in India of which almost all manufacturers are developing AHF in addition to others. Till date, no article is published to give detailed information about the herbal preparations on diabetes available in the market. In this, we illustrate about diabetes mellitus and its types, causes, sign, and symptoms, complications, pathophysiology, diabetic medication, diabetic treatment, herbal diabetic cure, advantages of herbal medicines over Allopathy and herbal formulations. Thus, this review article undertakes the attempt for providing updated information on the type of diabetes and herbal formulations which will enhance the existing knowledge of the researchers.
| Keywords: |
Diabetes mellitus, Anti-diabetic herbal formulations, Polyherbal formulations
INTRODUCTION: WHO defined Diabetes mellitus as “a metabolic disorder of multiple etiologies characterized by chronic hyperglycemia with disturbances in carbohydrate, fat and protein metabolism resulting from defects in insulin secretion, insulin action, or both” 1. The effects of diabetes mellitus include long-term damage, dysfunction, and failure of various organs including the kidney, nerves, heart and gastrointestinal tract.
It is the most common endocrine disorder worldwide with an incidence varying between 1 to 8% 2. The global prevalence of diabetes is estimated to increase, from 4% in 1995to 5.4% by the year 2025. 3 Despite the advancement in the synthetic anti-diabetic drugs in the recent past; diabetes is still remarkably not cured successfully. Treatment of diabetes is complicated due to the lack of drugs with safety and efficacy and is incapable of sustained clinical, biochemical, and histological cure.
On the contrary, the herbal drugs have gained wider importance worldwide, mostly due to higher safety, less number of adverse effects and consistent blood glucose lowering capacity. In the developed countries, the use of herbal medicine for the people with diabetes is encouraged by the concern about the adverse effects and cost associated with chronic use of the synthetic drug. There are wide ranges of phytoconstituents useful in the treatment of diabetes. These include alkaloids, glycosides, peptidoglycan, hypoglycin, steroids, guanidine, glycopeptides, terpenoides, amino acids, and inorganic ions. According to the ethnobotanical survey, there are about 800 plants which possess anti-diabetic potential 4.
Diabetes Mellitus: It is a metabolic disorder in the endocrine system. Diabetes is a chronic disorder in the metabolism of carbohydrate, proteins, and fat due to an absolute or relative deficiency of insulin secretion with/without a varying degree of insulin resistance. Also, it may be defined as a disease where the body produces little insulin / ceases to produce insulin or becomes progressive resistance to its actions 5, 6. It occurs worldwide, and the incidences of both type 1 and type 2 diabetes are rising; it is estimated that in the year 2000, 171 million people had diabetes, and this is expected to double by 2030. 7
Classification of Diabetes Mellitus:
1. β- cell destruction (Type 1 diabetes - IDDM)
(a) Immune mediated
(b) Idiopathy
2. Insulin resistance (Type 2 diabetes - NIDDM)
3. Genetic defects of β- cell function
(a) Glucokinase
(b) Hepatocyte nuclear transcription factor – 4 α
(c) Insulin promoter factor
(d) Mitochondrial DNA
(e) Proinsulin or insulin conversion
4. Genetic defects in insulin processing or insulin actions defects in
(a) Proinsulin conversion.
(b) Insulin gene mutation
(c) Insulin receptor mutation
5. Exocrine pancreatic defects
6. Endocrinopathy
(a) Acromegaly
(b) Cushing syndrome
(c) Hyperthyroidism
(d) Pheochrmocytoma
(e) Glucocanonama
7. Infections
(a) Cytomegalovirus
(b) Coxhacivirus
8. Drugs
(a) Glucocorticoid
(b) Thyroid hormone
(c) Thiazides
(d) Phenytoins
9. A genetic syndrome associated with diabetes
(a) Down’s syndrome
(b) Kleinfelter’s syndrome
(c) Turner’s syndrome
10. Gestational diabetes mellitus 8
Types of Diabetes: There are three main types of diabetes:
Type 1 Diabetes: Insulin - dependent diabetes (IDDM; Type I diabetes) is one of the most serious metabolic disorders, It has an autoimmune basis and is characterized by destruction of the pancreatic beta cells. Genetic and environmental factors play a part, and it is no surprise that HLA-DR3 and HLA-DR4 confer susceptibility to Type 1 diabetes mellitus 9.
Type 2 Diabetes: It formerly referred to as non-insulin-dependent diabetes mellitus, NIDDM for short, and adult-onset diabetes. Type 2 diabetes mellitus consists of an array of dysfunctions characterized by hyperglycemia and resulting from the combination of resistance to insulin action, inadequate insulin secretion, and excessive or inappropriate glucagon secretion 10.
Gestational Diabetes: Gestational diabetes mellitus (GDM) affects ∼ 7% of all pregnancies and is defined as carbohydrate intolerance during gestation. It is crucial to detect women with GDM because the condition can be associated with several maternal and fetal complications, such as macrosomia, birth trauma, cesarean section, and hypocalcemia, hypoglycemia & hyperbilirubinemia in newborns 11.
Causes of Diabetes: Multi-factorial, involving several predisposing conditions and risk factors. In many cases, genetics, habits, and environment may all contribute to a person’s diabetes.
Type 1 Diabetes: Type 1 diabetes is believed to be an autoimmune disease. The body's immune system specifically attacks the cells in the pancreas that produce insulin.
- A predisposition to developing Type 1 diabetes may run in families, but genetic causes (a positive family history) are much more common for Type 2 diabetes.
- Environmental factors, including common, unavoidable viral infections, may also contribute to Type 1 diabetes.
- Type 1 diabetes is most common in people of Non-Hispanic, Northern European descent, followed by African Americans, and Hispanic Americans.
- Type 1 diabetes is slightly more common in men than in women.
Type 2 Diabetes:
- High blood pressure.
- High blood triglyceride (fat) levels.
- Gestational diabetes or giving birth to a baby weighing more than 9 pounds.
- High-fat diet.
- High alcohol intake.
- Sedentary lifestyle.
- Obesity or being overweight.
- 12, 13
Signs and Symptoms: 14, 15, 16 Early detection and treatment of diabetes can decrease the risk of developing complications of diabetes. The following symptoms of diabetes are typical. However, some people with type 2 diabetes have symptoms so mild that they go unnoticed. Common symptoms of diabetes:
- Feeling very thirsty.
- Feeling very hungry - even though you are eating.
- Extreme fatigue.
- Blurry vision.
- Cuts / bruises that is slow to heal.
- Weight loss - even though you are eating more (Type 1).
- Tingling, pain, or numbness in the hands/feet (Type 2).
TABLE 1: SIGN AND SYMPTOMS OF DIABETES MELLITUS
| Pre-diabetes | Type 1 diabetes | Type 2 diabetes |
| No symptoms | Increased or extreme thirst | Increased thirst |
| Increased appetite | Increased appetite | |
| Increased fatigue | Fatigue | |
| Increased or frequent urination | Increased urination | |
| Unusual weight loss | weight loss | |
| Blurred vision | Blurred vision | |
| Fruity odor or breath | Sores that do not heal | |
| In some cases no symptoms | In some cases no symptoms |
Complications of Diabetes: The complications of diabetes mellitus are far less common and less severe in people who have well-controlled blood sugar levels 17, 18.
- Micro vascular Complications:
- Diabetic Retinopathy
- Diabetic Nephropathy
- Diabetic Neuropathy
- Macro vascular Complications:
- Atherosclerosis
- Cardiovascular Disease (CVD)
- Stroke
Pathophysiology of Diabetes: Mechanism of insulin release in normal pancreatic β cells - insulin production is more or less constant within the β cells. Its release is triggered by food, chiefly food containing absorbable glucose. Insulin is the principal hormone that regulates uptake of glucose from the blood into mast cells. Therefore, deficiency of insulin or the insensitivity of its receptors plays a central role in all forms of diabetes mellitus.
Humans are capable of digesting some carbohydrates, in particular, those most common in food; starch, and some disaccharides such as sucrose, are converted within a few hours to simpler forms, most notably the monosaccharide glucose, the principal carbohydrate energy source used by the body. The rest is passed on for processing by gut flora largely in the colon. Insulin is released into the blood by β cells (β-cells), found in the islets of langerhans in the pancreas, in response to rising levels of blood glucose, typically after eating. Insulin is used by about two-thirds of the body's cells to absorb glucose from the blood for use as fuel, for conversion to other needed molecules, or storage.
Insulin is also the principal control signal for conversion of glucose to glycogen for internal storage in liver and muscle cells. Lowered glucose levels result both in the reduced release of insulin from the β-cells and the reverse conversion of glycogen to glucose when glucose levels fall. This is mainly controlled by the hormone glucagon, which acts oppositely to insulin. Glucose thus forcibly produced from internal liver cell stores re-enters the bloodstream; muscle cells lack the necessary export mechanism.
Normally, liver cells do this when the level of insulin is low. Higher insulin levels increase some anabolic processes, such as cell growth and duplication, protein synthesis, and fat storage. Insulin is the principal signal in converting many of the bidirectional processes of metabolism from a catabolic to an anabolic direction, and vice versa. If the amount of insulin available is insufficient, if cells respond poorly to the effects of insulin or if the insulin itself is defective, then glucose will not have its usual effect, so it will not be absorbed properly by those body cells that require it, nor will it be stored appropriately in the liver and muscles. The net effect is persistent high levels of blood glucose, poor protein synthesis, and other metabolic derangements, such as acidosis.
When the glucose concentration in the blood is raised beyond its renal threshold, re-absorption of glucose in the proximal renal tubuli is incomplete, and part of the glucose remains in the urine (glycosuria), This increases the osmotic pressure of the urine and inhibits reabsorption of water by the kidney, resulting in increased urine production (Polyuria) 5, 19.
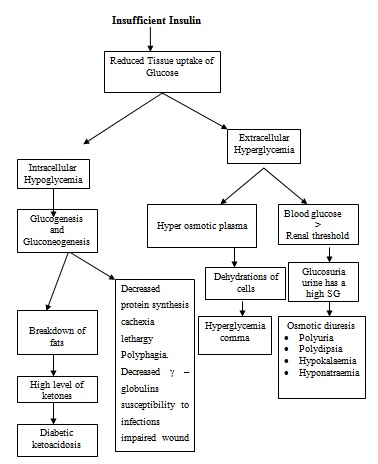
FIG. 1: PATHOGENESIS OF DIABETES MELLITUS 20
Diabetes Diagnosis: The blood glucose levels of a healthy man are 80 mg/dL on fasting and up to 160 mg/dL in the postprandial state.
Some laboratory tests are available to confirm the diagnosis of diabetes.
- Finger Stick Blood Glucose.
- Fasting Plasma Glucose.
- Oral Glucose Tolerance Test.
- Glycosylated Hemoglobin or Hemoglobin A1c15.
Who Diabetes Diagnostic Criteria: 21, 22
TABLE 2: DIAGNOSTIC CRITERIA OF DIABETES MELLITUS
| Condition | 2 h Glucose | Fasting glucose | Hb A1c |
| Unit | mmol/l(mg/dl) | mmol/l (mg/dl) | % |
| Normal | <7.8 (<140) | <6.1 (<110) | <6.0 |
| Impaired fasting glycaemia | <7.8 (<140) | ≥6.1(≥110) & <7.0 (<126) | 6.0–6.4 |
| Impaired glucose tolerance | ≥7.8 (≥140) | <7.0 (<126) | 6.0–6.4 |
| Diabetes mellitus | ≥11.1 (≥200) | ≥7.0 (≥126) | ≥6.5 |
Diabetes Medications: Many different types of medications are available to help lower blood sugar levels in people with Type 2 diabetes. Each type works differently. It is very common to combine two or more types to get the best effect with fewest side effects.
Sulfonylurea: These drugs stimulate the pancreas to make more insulin.
Biguanides: These agents decrease the amount of glucose produced by the liver.
Alpha-Glucosidase Inhibitors: These slow agent absorption of the starches and glucose.
Thiazolidinediones: These agents increase sensitivity to insulin.
Meglitinides: These agents stimulate the pancreas to make more insulin.
D-phenylalanine Derivatives: These agents stimulate the pancreas to produce more insulin more quickly.
Amylin Synthetic Derivatives: Amylin is a naturally occurring hormone secreted by the pancreas along with insulin. An amylin derivative, such as pramlintide (Symlin), is indicated when blood sugar control is not achieved despite optimal insulin therapy.
Incretin Mimetics: Exenatide (Byetta) was the first incretin mimetic agent approved in the United States. It is indicated for diabetes mellitus type 2 in addition to metformin or a sulfonylurea when these agents have not attained blood sugar level control alone.
Insulins: Synthetic human insulin is now the only type of insulin. It is less likely to cause allergic reactions than animal-derived varieties of insulin used in the past. Different types of insulin are available and categorized according to their times of action onset and duration.
- Examples of Rapid-Acting Insulins:
Regular insulin (Humulin R, Novolin R):
- Insulin lispro (Humalog).
- Insulin aspart (Novolog).
- Insulin glulisine (Apidra).
- Prompt insulin zinc (Semilente, slightly slower acting).
- Examples of Intermediate-Acting Insulins:
- Isophane insulin, neutral protamine Hagedorn (NPH) (Humulin N, Novolin N).
- Insulin zinc (Lente).
- Examples of long-acting insulins –
- Extended insulin zinc insulin (Ultralente).
- Insulin glargine (Lantus).
- Insulin detemir (Levemir) 23, 24.
Diabetes Treatment: Treatment involves medicines, diet, and exercise to control blood sugar and prevent symptoms and problems 25.
Diabetes Diet: A healthy diet is key to controlling blood sugar levels and preventing diabetes complications.
- If the patient is obese and had difficulty losing weights on their own then talk to a health care professional or dietitian.
- Eat a consistent, well-balanced diet that is high in fiber, low in saturated fat, and low in concentrated sweets.
- A consistent diet that includes roughly the same number of calories at about the same times of the day.
Exercise: Regular exercise, in any form, can help reduce the risk of developing diabetes. Activity can also reduce the risk of developing complications of diabetes such as heart disease, stroke, kidney failure, blindness, and leg ulcers.
- As little as 20 min of walking three times a week have a proven beneficial effect.
- If the patient has complications of diabetes (such as eye, kidney, or nerve problems), they may be limited both in the type of exercise, and amount of exercise they can safely do without worsening their condition. Consult with your health care professional before starting any exercise program.
Alcohol Use: Moderate or eliminate consumption of alcohol. Excessive alcohol use is a known risk factor for type 2 diabetes. Alcohol consumption can cause low or high blood sugar levels, nerve pain (neuritis), and an increase in triglycerides.
Smoking: If the patient has diabetes, and smokes cigarettes or use any other form of tobacco, they are raising the risks. Smoking damages blood vessels and contributes to heart disease, stroke, and poor circulation in the limbs. If a person needs help to quit tobacco use, talk to a health care professional.
Self-Monitored Blood Glucose: Check blood sugar levels frequently, at least before meals and at bedtime, then record the results in a logbook.
- This log should also include insulin or oral medication doses and times, when and what the patient ate, when and for how long they exercised, and any significant events of the day such as high or low blood sugar levels and how they treated the problem.
- Better equipment now available makes testing blood sugar levels.
Education: When the patient is first diagnosed with diabetes, the diabetes care team will spend a lot of time with the patient, teaching them about their condition, treatment, and everything they need to know to care for them on a daily basis.
Diabetes Follow-Up: Follow the health care professional's treatment recommendations.
- Keep records of blood sugar levels as often as recommended by the health care professional.
- Call the health care professional if the patient has any problems with their treatment or symptoms that suggest poor glucose control.
Diabetes Prevention: It is not yet known how to prevent type 1 diabetes. Type 2 diabetes, however, can be prevented in some cases.
- Control weight to normal or near-normal levels by eating a healthy low-fat, high-fiber diet.
- Regular exercise is crucial to the prevention of type 2 diabetes.
- Keep alcohol consumption low.
- Quit smoking.
- If a person has high blood fat levels (such as high cholesterol) or high blood pressure, take all medications as directed.
- Lifestyle modifications and certain medications can be used in people with prediabetes to prevent progression to diabetes.
- Tight glucose control: The single best thing a person with diabetes can do is to keep their blood sugar level within the suggested range every day.
- Quit smoking
- Maintain a healthy weight
- Increase physical activity levels.
- Drink an adequate amount of water and avoid consuming too much salt.
- The skin should be taken care of; keep it supple and hydrated to avoid sores and cracks that can become severely infected.
- Brush and floss the teeth every day.
- The feet should be washed and examined daily, looking for small cuts, sores, or blisters that may cause problems later.
Herbal Diabetes Cure: Herbs for diabetes treatment are not new. Since, ancient times, plants and plant extracts were used to combat diabetes. Here are some herbs that have been confirmed by scientific investigation, which appear to be most effective, relatively non-toxic and have substantial documentation of efficiency 7, 26.
Cinnamon: Cinnamon is the inner bark of a tropical evergreen tree native to India and Sri Lanka. It has insulin-like properties, which able to decrease blood glucose levels as well as triglycerides and cholesterol, all of which are important especially for type 2 diabetes patients.
Pterocarpus marsupium: It is a large deciduous tree. Pterocarpus marsupium demonstrates to reduce the glucose absorption from the gastro-intestinal tract, and improve insulin and pro-insulin levels. It also effective in β cell regeneration.
Bitter Melon (Momordica charantia): Also known as bitter gourd, bitter cucumber, karela, and charantin. Studies suggested that Asian Bitter Melon may lower blood glucose concentrations. Several compounds have been isolated from bitter melon that is believed to be responsible for its blood-sugar-lowering properties. These include charantin and an insulin-like protein referred to as polypeptide-P, or plant insulin. It is believed that bitter melon acts on both the pancreas and in non-pancreatic cells, such as muscle cells.
Gymnema sylvestre: To treat diabetes, dried leaves are powdered together with coriander fruit juice is extracted and given orally. These remedy has been used in India for treating diabetes for about 2000 years. Today in India it is being used to treat primarily type II diabetes and type I as well. Gymnema also improves the ability of insulin to lower blood sugar in both types I and type II diabetes. This herb is showing up in more and more over the counter weight loss products and blood sugar balancing formulas.
Onion: Onion is a member of the lily family (Liliaceae). Experimental and clinical evidence suggests that onion consists of an active ingredient called APDS (allyl propyl disulfide). APDS has been shown to block the breakdown of insulin by the liver and possibly to stimulate insulin production by the pancreas, thus increasing the amount of insulin and reducing sugar levels in the blood. The additional benefit of the use of garlic is its beneficial cardiovascular effects. It is found to lower lipid levels, inhibit platelet aggregation and are antihypertensive. So, the use of onion is recommended for diabetes patients.
Fenugreek (Trigonella foenum - ngraecum): Fenugreek or frenum-graecum, is a crop plant grown as a potherb and for the spice made from its seeds. The fenugreek plant grows wild from the eastern Mediterranean area to China; it cultivated worldwide. Fenugreek is used both as an herb (the leaves) and as a spice (the seed). Pre-clinical and clinical studies have demonstrated the anti-diabetic properties of fenugreek seeds. The fiber-rich fraction of fenugreek seeds can lower blood sugar levels in people with diabetes, and to a lesser extent, for lowering blood cholesterol. Additionally, the soluble fiber content of fenugreek may play a role in aiding weight control.
Blueberry (Vaccinium myrtillus): They are closely related to the European bilberry. There are several species of blueberries exist-including V. pallidum and V. corymbosum and grow throughout the United States. Its leaves are the primary part of the plant used medicinally.
Blueberry is a natural method of controlling or lowering blood sugar levels the leaves have an active ingredient with a remarkable ability to get rid the body of excessive sugar in the blood. It is a good astringent and helps relieve inflammation of the kidney, bladder, and prostate.
Asian Ginseng: Asian ginseng is commonly used in traditional Chinese medicine to treat diabetes. It has been shown to enhance the release of insulin from the pancreas and to increase the number of insulin receptors. It also has a direct blood sugar-lowering effect and improves psycho-physiological performance.
Ginkgo biloba: Long used in traditional Chinese medicine, a species that has survived in China for more than 200 million years and now grows throughout the world. This popular herbal medicine is extracted from the fan-shaped leaves of the ancient Ginkgo biloba tree. The extract may prove useful for the prevention and treatment of early-stage diabetic neuropathy. Gingko biloba extract improves blood flow in the peripheral tissues of the nerves in the arms, legs, hands, and feet and is, therefore, an important medicine in the treatment of peripheral vascular disease. It has also been shown to prevent diabetic retinopathy.
Banaba (Lagerstroemia speciosa): Banaba is a variety of crepe myrtle that grows in the Philippines, India, Malaysia, and Australia. Banaba possesses the powerful compound corosolic acid and tannins, including lagerstroemia that lends itself to the treatment of diabetes. These ingredients are thought to stimulate glucose uptake and have insulin-like activity. The latter activity is thought to be secondary to activation of the insulin receptor tyrosine kinase or the inhibition of tyrosine phosphatase. It is natural plant insulin, can be taken orally.
Babul (Acacia arabica): It is found all over India mainly in the wild habitat. The plant extract acts as an anti-diabetic agent by acting as secretagogue to release insulin.
Bengal Quince, Bel or Bilva (Aegle marmelos): Administration of aqueous extract of leaves improves digestion and reduces blood sugar and urea, serum cholesterol. Along with exhibiting hypoglycemic activity, this extract also prevented peak rise in blood sugar at 1h in oral glucose tolerance test.
Garlic (Allium sativum): This is a perennial herb cultivated throughout India. Allicin, a sulfur-containing compound is responsible for its pungent odor and it has been shown to have significant hypoglycemic activity. This effect is thought to be due to increased hepatic metabolism, increased insulin release from pancreatic β cells and insulin-sparing effect, thus decreased fasting blood glucose, and triglyceride levels in serum in comparison to sucrose controls.
S-allyl cysteine sulfoxide (SACS), the precursor of allicin and garlic oil, is a sulfur-containing amino acid, which controlled lipid peroxidation better than glibenclamide and insulin. It also improved diabetic conditions. SACS also stimulated In-vitro insulin secretion from beta cells isolated from normal rats. Apart from this, Allium sativum exhibits antimicrobial, anticancer and cardio-protective activities.
Aloe (Aloe vera and Aloe barbadensis): Aloe, a popular houseplant, has a long history as a multipurpose folk remedy. The plant can be separated into two basic products: gel and latex. Aloe vera gel is the leaf pulp or mucilage, aloe latex, commonly referred to as “aloe juice,” is a bitter yellow exudate from the pericyclic tubules just beneath the outer skin of the leaves. Extracts of aloe gum effectively increase glucose tolerance in both normal and diabetic rats.
Treatment of chronic but not a single dose of exudates of Aloe barbadensis leaves showed hypoglycemic effect. Single, as well as chronic doses of the bitter principle of the same plant, also showed hypoglycemic effect. This action of Aloe vera and its bitter principle is through stimulation of synthesis and release of insulin from pancreatic beta cells. This plant also has anti-inflammatory activity in a dose-dependent manner and improves wound healing in diabetes.
Neem (Azadirachta indica): Hydroalcoholic extracts of this plant showed anti-hyperglycemic activity. Apart from having anti-diabetic activity, this plant also has anti-bacterial, anti-malarial, anti-fertility, hepatoprotective and antioxidant effects.
Caesalpinia bonducella: Caesalpinia bonducella is widely distributed throughout the coastal region of India and used ethnically by the tribal people of India for controlling blood sugar. Both the aqueous and ethanolic extracts showed potent hypoglycemic activity in chronic type II diabetic models. These extracts also increased glycogenesis thereby increasing liver glycogen content. The anti-hyperglycemic action of the seed extracts may be due to the blocking of glucose absorption. The drug has the potential to act as anti-diabetic as well as anti-hyperlipidemic.
Indian Goose Berry, Jamun (Eugenia jambolana): In India decoction of kernels of Eugenia jambolana is used as a household remedy for diabetes. This also forms a major constituent of many herbal formulations for diabetes.
Anti-hyperglycemic effect of aqueous and alcoholic extract, as well as lyophilized powder, shows a reduction in blood glucose level. This varies with the different level of diabetes. The extract of jamun pulp showed the hypoglycemic activity in streptozotocin-induced diabetic rats. These extracts also inhibited insulinase activity from liver and kidney.
Mango (Mangifera indica): The leaves of this plant are used as an anti-diabetic agent in Nigerian folk medicine, although when aqueous extract given orally did not alter blood glucose level in either normoglycemic or streptozotocin-induced diabetes. The aqueous extract of Mangifera indica possesses hypoglycemic activity. This may be due to an intestinal reduction of the absorption of glucose.
Holy Basil (Ocimum sanctum):It is commonly known as Tulsi. Since ancient times, this plant is known for its medicinal properties. The aqueous extract of leaves of Ocimum sanctum showed the significant reduction in blood sugar level in both normal and alloxan-induced diabetes. Significant reduction in fasting blood glucose, uronic acid, total amino acid, total cholesterol, triglyceride, and total lipid indicated the hypoglycemic and hypolipidemic effects of tulsi in diabetes.
This plant also showed anti-asthemitic, anti-stress, anti-bacterial, anti-fungal, anti-viral, anti-tumor, gastric anti-ulcer activity, anti-oxidant, anti-mutagenic and immunostimulant activities.
Bhuiamala (Phyllanthus amarus): It is a herb of height up to 60 cm, from family Euphorbiaceae. It is commonly known as Bhuiamala. It is scattered throughout thehotter parts of India, mainly Deccan, Konkan, and south Indian states. Traditionally it is used in diabetes therapeutics. Methanolic extract of Phyllanthus amarus was found to have potent antioxidant activity. This extract also reduced the blood sugar in alloxanized diabetes. The plant also shows anti-inflammatory, anti-mutagenic, anti-carcinogenic, anti-diarrhoeal activity.
Polyherbal Formulation: Major formulations used in Ayurveda are based on herbs used as decoctions, infusion, tinctures, and powders. Drug formulation in Ayurveda (As mention in Ayurvedic treatise like Charaka Samhita, Sushruta Samhita) is based on two principles: (a). Use as a single drug, and (b). Use of more than two drugs. When two or more herbs are used in formulation, they are known as polyherbal formulation.27 Different polyherbal formulations available in the market:
Dihar: A polyherbal formulation containing eight different herbs Syzygium cumini, Momordica charantia, Emblica officinalis, Gymnema sylvestre, Enicostemm, Azadirachta indiaca, Tinospora cordifolia and Curcuma longa. Literature revealed that the combination of these eight herbs shows effective anti-hyperglycemic activity in streptozotocin (STZ, 45 mg/kg i.v single dose) induced type 1 diabetic rats. Treatment with Dihar (100 mg/kg) for 6 weeks produced a decrease in STZ induced serum glucose and lipid levels and increases insulin levels as compared to control. Dihar produced a significant decrease in serum creatinine urea level and lipid peroxidation in diabetic rats. Administration of Dihar to diabetic rats significantly increased the activity of antioxidant enzyme 28.
Diabet: A polyherbal formulation containing Curcuma longa, Coscinium fenestratum, Strychnos potatorum, Phyllanthus reticulates, Tamarindus indica, Tribulus terrestris was investigated for its glucose tolerance and anti-diabetic activity in alloxan-induced diabetic rats. The glucose tolerance test and hypoglycemic studies carried out in normal rats at a dose of 500 mg/kg. The product showed its effectiveness at a dose of 500 mg/kg but does not hypoglycemic effect 27.
Diasol: A polyherbal anti-diabetic formulation containing plant extracts of Eugenia jambolana, Foenum graceum, Terminalia chebula, Quercus, infectoria, Cuminum cyminum, Taraxacum officinale, Emblica officinalis, Gymnea sylvestre, Phyllanthus niruri and Enicostemma littorale. Previous investigation showed Diasol reduces 63.4% of blood glucose level in a dose of 125 and 250 mg/kg b.w (i.p) and proved to be effective anti-diabetic polyherbal formulation 29.
Dianex: A polyherbal formulation was screened for antidiabetic activity in rats, and it has been reported that Dionex produces significant hypoglycemic activity in both normal and diabetic mice. It was administered orally in different doses of 100, 250 and 500 mg/kg b.w up to 6 weeks 30.
Diashis: A study was conducted on polyherbal formulation composed of eight medicinal plants for the management of streptozotocin (STZ)-induced diabetes in rats. As oxidative stress is one of the consequences of diabetes, the activities of hepatic antioxidant enzymes and metabolic enzymes were evaluated. The study revealed that treatment with 'Diashis' in STZ-induced diabetic rats resulted in a significant recovery in the activities of hepatic hexokinase, glucose-6-phosphate dehydrogenase, and glucose-6-phosphatase along with the correction in the levels of fasting blood glucose, glycated hemoglobin, liver, and skeletal muscle glycogen. The oxidative stress status in the liver was corrected by 'Diashis' which was highlighted by the recovery in the activities of catalase, peroxidase, and glutathione-S-transferase along with the correction in the quantity of thiobarbituric acid reactive substances and a conjugated diene. 'Diashis' was not found to have any metabolic toxicity 31.
Diabrid: A herbal based anti-diabetic formulation for maturity onset diabetic patients were clinically evaluated in 60 diabetic patients for six months. The clinical studies revealed that Diabrid was well tolerated in high doses and was found to be a potential anti-diabetic drug in mild and moderate diabetic cases (180-280 mg/dl). The blood sugar level was controlled within a 2-8 week depending upon initial blood sugar level. No side effect was observed. The hypoglycemic activity was dose-dependent and gradual. The drug also maintained the body weight and blood pressure of diabetic patients. No deleterious effect was observed on the kidney and liver 32.
Diakyur: A polyherbal formulation (composed of Cassia javanica, Cassia auriculata, Salacia reticulate, Gymnema sylvestre, Mucuna pruriens, Syzygium jambolana and Terminalia arjuna) scientifically proved to be a potential antidiabetic formulation in previous studies. It indicated that Diakyur had shown significant hypoglycemic activity as well as anti lipid peroxidative activity so that it can be used as an adjuvant along with allopathic treatment of medicine to treat diabetes as well as to delay the late complications of diabetes. So, concluded that Diakyur at a dose of 1600 mg/kg p.o is safe for long term treatment in diabetic condition 33.
Diasulin: A polyherbal formulation containing Cassia auriculata, Coccinia indica, Curcuma longa, Emblica officinalis, Gymnema sylvestre, Momordica charantia, Scoparia dulcis, Syzygium cumini, Tinospora cordifolia, Trigonella foenum graecum. Previous investigation suggest that controls the blood glucose level by increasing glycolysis and decreasing gluconeogenesis with a lower demand for pancreatic insulin than in untreated rats. This is possible because it regulates the activities of hepatic glucose metabolic enzymes. Diasulin also resulted in a significant decrease in tissue lipids and lipid peroxide formation 34.
Diabecon: A polyherbal formulation containing Gymnema sylvestre, Pterocarpus marsupium, Glycyrrhiza glabra, Casearia esculenta, Syzygium cumini, Asparagus racemosus, Boerhavia diffusa, Sphaeranthus indicus, Tinospora cordifolia, Swertia chirata, Tribulus terrestris, Phyllanthus amarus, Gmelina arborea, Gossypium herbaceum, Berberis aristata, Aloe vera, Triphala, Commiphora wightii, shilajeet, Momordica charantia, Piper nigrum, Ocimum sanctum, Abutilon indicum, Curcuma longa, Rumex maritimus is reported to increase peripheral utilization of glucose, increase hepatic and muscle glucagon contents, promote B cells repair and regeneration and increase C- peptide level. It has antioxidant properties and protects β cells from oxidative stress. It exerts insulin-like action by reducing the glycated hemoglobin levels, normalizing the microalbuminuria and modulating the lipid profile. It minimizes long term diabetic complications.
Previous studies also revealed than Diabecon is a safe drug to prevent complications such as retinopathy in diabetic patients. Diabecon resolved retinal and vitreal hemorrhages and its subsequent prevention. It also enhanced the absorption of hard and soft exudates by anti-inflammatory properties Studies concluded that Diabecon could be used as an adjuvant with conventional treatment in NIDDM and IDDM patients 35.
Dia-Care: A herbal formulation containing Sanjeevan Mool; Himej, Jambu beej, Kadu, Namejav, Neem chal is claimed to be effective for both Type 1, Type 2 diabetes within 90 days of treatment and cures within 18 months. Persons taking insulin will eventually be liberated from the dependence it.
The whole treatment completes in 6 phases, each phase being of 90 days. Approx. 5 gm (1 teaspoon) powder is mixed with 1/2 glass of water, stirred properly, kept overnight and filtered. The filtrate is taken in the morning on an empty stomach. To the remaining medicine fresh water is added and kept for the whole day and is consumed half an hour before dinner. The taste of the drug is very bitter. It is a pure herbal formula without any side effect 36.
Diabetes-Daily Care: Diabetes - daily care containing alpha lipoic acid, cinnamon 4% extract, chromax, vanadium, fenugreek 50% extract, Gymnema sylvestre 25% extract, Momordica 7% extract, Licorice root 20% extract is a unique, natural formula, which effectively and safely improves sugar metabolism 37.
Diabecure: A formulation containing Juglans regia, Berberis vulgaris, Erytherea centaurium, Millefolium, Taraxacum effective in lowering the blood sugar level 38.
Diabeta: A formulation containing Gymnema sylvestre, Vinca rosea (Periwinkle), Curcuma longa (Turmeric), Azadirachta indica (Neem), Pterocarpus marsupium (Kino Tree), Momordica charantia (Bitter Gourd), Syzygium cumini (Black Plum), Acacia arabica (Black Babhul), Tinospora cordifolia, Zingiber officinale (Ginger) available in the capsule form is an anti-diabetic with combination of proven anti-diabetic fortified with potent immunomodulators, anti-hyperlipidemic, anti-stress and hepatoprotective of plant origin.
The formulation of Diabeta is based on ancient ayurvedic references, further corroborated through modern research and clinical trials. Diabeta acts on different sites in differing ways to effectively control factors and pathways leading to diabetes mellitus. It attacks the various factors, which precipitate the diabetic condition, and corrects the degenerative complications, which result because of diabetes. Diabeta is safe and effective in managing Diabetes mellitus as a single agent supplement to synthetic anti-diabetic drugs.
Diabeta helps overcome resistance to oral hypoglycemic drugs when used as an adjuvant to cases of uncontrolled diabetes. Diabeta confers a sense of well-being in patients and promotes symptomatic relief of complaints like weakness giddiness, pain in legs, body ache, polyuria and pruritis 39.
Glyoherb: A polyherbal formulation was evaluated for its antihyperglycemic, antihyperlipidemic and anti-oxidant effects against normal and streptozotocin-induced diabetic rats. ‘Glyoherb’ sugar control granules possess potential anti-diabetic activity as it lowers serum glucose levels and increases glucose tolerance in STZ-induced Type 1 diabetic rats. This polyherbal formulation also possesses significant antihyperlipidemic activity as it lowers serum cholesterol and triglyceride levels. ‘Glyoherb’ did not exert any toxic effects in STZ-induced impaired kidney and liver functions. It was rather found to be improving kidney and liver functions.
Also, ‘Glyoherb’ possesses potential antioxidant activity as it decreases lipid peroxidation and enhances antioxidant status in diabetic rats. The antidiabetic activity of ‘Glyoherb’ may be attributed to its antioxidant properties also. Thus previous research concluded that ‘Glyoherb’ might be regarded as a promising natural and safe remedy for the prevention or delay of diabetic complications 40.
Karmin Plus: An indigenous polyherbal formulation containing Momordica charantia, Azadirachta indica, Picrorrhiza kurroa, Ocimum sanctum, and Zingiber officinale was evaluated for antidiabetic activity, and it was found that product showed effectiveness at two dose levels at 200 mg/kg and 400 mg/kg b.w for anti-diabetic activity 41.
Okuda et: Studies on a formulation containing Stachytarpheta angustifolia, Alstonia congensis bark, and Xylopia acthiopica fruits extract showed that polyherbal formulation was effective in decreasing plasma glucose levels in the diabetic rats and proved to have better plasma glucose lowering effect that glibenclamide and also having a good reducing effect on Cardiovascular system. The high LD50 value (16.5 g/kg) indicates that formulation could be safe for us 42.
Advantages of Herbal Medicines over Allopathy:
Natural Healing: herbal medicine doesn't obstruct the body's self-healing abilities in any way. On the contrary, they enhance the biological healing machinery so that the recovery process gets accelerated and the body can maintain an ideal internal environment that is crucial for such a recovery.
Continued Benefits: A lot of herbal remedies come with special instructions about diet, rest, and exercises that enhance the potency of the herb by preparing the body in such a way that it responds to the treatment most effectively and desirably. These dietary and lifestyle changes ultimately help the patient by getting their bodies into a healthy rhythm.
Better Immunity: Owing to their tendency of enhancing the body's natural healing process and correcting bad habits that lead to ill-health, herbs contribute towards strengthening the immune system.
Metabolism and Nutrition: A stronger immune system and a holistically regulated diet and lifestyle lead to improved metabolism, which in turn leads to better absorption of nutrition from one's diet.
Side Effects: Side effects the contraindications are minimal when herbal medication is taken as per prescription and under the supervision of a qualified practitioner 43.
CONCLUSION: The present study aims to give complete information about diabetes and herbal polyherbal formulations available in the market for diabetes that are the alternatives to synthetic medicines. Herbal medication of diabetes is much better than allopathy.
ACKNOWLEDGEMENT: Nil
CONFLICT OF INTEREST: Nil
REFERENCES:
- Report of a WHO Consultation. Part 1: Definition, diagnosis and classification of Diabetes complications cited in Geneva, World Health Organization 1999.
- Haller H, Drab M and Luft FC: The role of hyperglycemia and hyperinsulinemia in the pathogenesis of diabetic angiopathy. Clin Nephrol 1996; 46(4): 246-55.
- King H, Aubert RE and Herman WH: Global burden of diabetes 1995-2025; Prevalence, numerical estimates, and projection. Diabetes Care 1998; 21: 1414-31.
- Alarcon AFJ, Roman RR, Perez GS, Aguilar CA, Contreras WCC and Flores SJL: Study of the anti-hyperglycemic effect of plants used as anti-diabetics. J Ethno Pharm 1998; 61: 101-10.
- Barar FSK: Essentials of Pharmacotherapeutics. S. Chand & Company Ltd, Edition 4th, 2008: 340-349.
- Brunton LL, Lazo SJ and Parker LK: Goodman & Gilman’s: The Pharmacological basis of Therapeutics. Mc Graw Hill Company, Edition 10th, 2001.
- Jarald E, Joshi SB and Jain DC: Diabetes & herbal medicines: review article. Iranian Journal of Pharmacology & Therapeutics 2008; 7: 97-106.
- Harsh M: Text Book of Pathology. J.P. Brothers, Edition 5th, 2005:843.
- Hober D and Alidjinou EK: Enteroviral pathogenesis of type 1 diabetes: queries and answers. Curr Opin Infect Dis 2013; 26: 263-9.
- Romesh K: Type 2 Diabetes mellitus. Medscape cited from www.emedicine.medscape.com/article.
- Jennifer MP: Perspectives in gestational diabetes mellitus: A review of screening, diagnosis, and treatment. Clinical Diabetes 2007; 25(2): 57-62.
- Riaz S: Diabetes mellitus: A review. Scientific Research & Essay 2009; 4: 367-373.
- Robert Ferry JR: Emedicinehealth [Internet]. [Place unknown]: Melissa Conrad Stopller; 2008 [cited 2012 Sep 9]. Available from: www. Emedicine health. com/ diabetes/article_em. htm.
- America heart Association Cited from http:// www. diabetes.org/diabetes-basics/symptoms.
- Wikipedia, The free encyclopedia. Diabetes mellitus. 2009 Nov. Available from: http:// en. Wikipedia. org/ Wiki/ Diabetes mellitus.
- D.A.M Medical Encyclopedia. America. Pubmed; 2012 Jun 27. Available from www.ncbi.nlm.nih.gov/pubmed health.
- Nathan DM, Cleary PA and Backlund JY: Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. The New England Journal of Medicine 2005; 353(25): 2643-53.
- Diabetes Complications. www.Diabetes.co.uk. 2012.
- Walker R and Whittlesea C: Clinical Pharmacology & Therapeutics. Churchill Livingstone, Edition 4th, 2008: 629-652.
- Cited from http://http://www.caninsulin.com.
- Definition and diagnosis of diabetes mellitus and intermediate hyperglycemia: report of a WHO/IDF consultation. Geneva: World Health Organization 2006.
- Vijan S: Type 2 diabetes. Annals of internal medicine 2010; 152(5): ITC31-15.
- Howland RD, Mycek MJ, Champe PC and Harvey RA: Pharmacology. UK: Lippincott Williams & Wilkins 2006: 281-294.
- Rang HP, Dale MM, Ritter JM and Flower RJ: Pharmacology. UK: Churchill Livingstone; Edition 4th, 2007: 402-404.
- Cited from http://www.emedicinehealth.com.
- Cited from http://,http://www.iloveindia.com/indian-erbs/herbs-for-diabetes.
- Shrivastava S, Lal VK and Pant KK: Polyherbal formulations based on Indian medicinal plants as anti-diabetic phytotherapeutics. Phytopharmacology 2012; 2(1): 1-15.
- Patel SS, Shah SS and Goyal RK: Antihyperglycemic, antihyperlipidemic and antioxidant effects of Dihar, a polyherbal ayurvedic formulation in streptozotocin-induced diabetic rats. Indian J Exp Biol 2009; 47(7): 564-70.
- Seevalen SHB, Debasish S, Vethambur B and Tajudeen K: Evaluation on safety and efficacy of a polyherbal antidiabetic formulation-DIASOL. As Pac J Mol Biol Biotechnol 2010; 18(1): 59-61.
- Mutalik S, Sulochana B, Devi UP and Udupu N: Preliminary studies on acute and subacute toxicity of an antidiabetic herbal preparation, Dianex. Indian Journal of Experimental Biology 2003; 41: 316-320.
- Tushar KB, Debasis D, Kausik C, Kazi MA and Debidas G: Effect of Diashis, a polyherbal formulation, in streptozotocin-induced diabetic male albino rats. Int J Ayurveda Res 2010; 1(1): 18-24.
- Qadri NM, Rehman Z and Shireen K: Evaluation of antidiabetic activity of Diabrid, a herbal formulation in Type-II diabetic patients. Jour Chem Soc Pak 2006; 28(3): 281-283.
- Joshi CS, Priya ES and Venkataraman: Hypoglycaemic anti-lipidperoxidative effects of a polyherbal formulation, Diakyur in experimental animal models. Journal of Health Sciences 2007; 53(6): 734-739.
- Pari L and Saravanan R: Anti-diabetic effect of diasulin, a herbal drug, on blood glucose, plasma insulin and hepatic enzymes of glucose metabolism in hyperglycaemic rats. Diabetes Obes Metab 2004; 6(4): 286-292.
- Mohan V: Evaluation of diabecon (D-400) as an anti-diabetic agent- a double-blind placebo-controlled trial in NIDDM patients with secondary failure to oral drugs. Indian Journal of Clinical Practice 1998; 9(8): 18.
- Reddy KS, Reddy YP and Devana N: Anti-diabetic activity of a polyherbal formulation (Dia-care). Adv. Pharmacol Toxicol 2012; 13(3): 27-30.
- Jonnalagadd VG and Selkar N: Anti-diabetic herbal products marketed in India: An update. Journal of Medicinal Plants studies 2013; 1(6): 24-26.
- Awasthi H, Mani DN, Nath R and Kumar S: Anti-hyperglycemic activity of polyherbal formulation and its protective role against hepatopathy in streptozotocin-induced diabetic rats. International Journal of Current Research 2013; 5(10): 3184-3191.
- Cited from http://www.ayurvediccure.com/.
- Thakkar NV and Patel J: Pharmacological evaluation of “Glyoherb”: A polyherbal formulation on streptozotocin-induced diabetic rats. Int J Diabetes Dev Ctries 2010; 30(1): 1-7.
- Bangar OP, Jarald EE, Asghar S and Ahmad S: Anti-diabetic Activity of a polyherbal formulation (Karmin plus). Int J Green Pharm 2009; 3: 211-214.
- Ogbonnia SO, Mbaka GO, Adekunle A, Anyika EN, Gbolade OE and Nwakakwa N: Effect of a poly-herbal formulation, okudiabet, on alloxan- induced diabetic rats. Agriculture and Biology Journal of North America 2010; 1(2): 139-145.
- Cited from http://www.OAWPolicy.com
How to cite this article:
Kaur M and Valecha V: Diabetes and anti-diabetic herbal formulations: an alternative to Allopathy. Int J Pharmacognosy 2014; 1(10): 615-27. doi link: http://dx.doi.org/10.13040/IJPSR.0975-8232.IJP.1(10).615-27.
This Journal licensed under a Creative Commons Attribution-Non-commercial-Share Alike 3.0 Unported License.
Article Information
1
615-627
784
3330
English
IJP
M. Kaur* and V. Valecha
Faculty of Pharmaceutical Sciences, Doon Valley Institute of Pharmacy And Medicines, Karnal, Haryana, India.
maninder3maninder@gmail.com
11 August 2014
08 September 2014
28 September 2014
http://dx.doi.org/10.13040/IJPSR.0975-8232.IJP.1(10).615-27
01 October 2014