


BIOMECHANICAL ALTERATIONS IN WOMEN WITH POLYCYSTIC OVARY SYNDROME: LINKING LUMBOPELVIC ALIGNMENT
HTML Full TextBIOMECHANICAL ALTERATIONS IN WOMEN WITH POLYCYSTIC OVARY SYNDROME: LINKING LUMBOPELVIC ALIGNMENT
Mohammad Sadam Lone, Ranjan Kumar Singh *, Tanya Sharma and Satpal Kushwaha
Department of Pharmacy, Mewar University, Gangrar, Chittorgarh, Rajasthan, India.
ABSTRACT: Polycystic ovary syndrome (PCOS) is a complex endocrine characterized by hyperandrogenism, hormonal imbalances, and metabolic disruptions, leading to reproductive complications and increased risk of cardiometabolic diseases. While lifestyle modifications are the cornerstone of PCOS management, pharmacological interventions, including metformin, oral contraceptives, and anti-androgens, are commonly utilized. Recently, glucagon-like peptide-1 receptor agonists (GLP-1 RAs) and sodium-glucose cotransporter-2 inhibitors (SGLT2is) have shown promising results in PCOS management. Polycystic ovarian syndrome (PCOS) is a prevalent endocrine disorder that causes an females with PCOS also experience chronic inflammation. This hormonal imbalance and persistent inflammation can reduce muscle strength and mass. Consequently, this may affect the lumbopelvic muscles, potentially leading to postural abnormalities and spinal misalignment. The study's goals were to find out how the biomechanics of women with PCOS differ from those who did not have the condition and to confirm the link between lumbopelvic parameters and the LH/FSH ratio in women with PCOS. The researcher conducted a case-control study on 95 nulliparous females, with 52 having PCOS and classified as a study group and 43 as a control group. The participants ranged in age from 25 to 35 years, and their body mass index ranged from 25 to 29.9 kg/m2. All participants were selected from the gynecological outpatient clinic of Om El-Masryeen Hospital. The researcher used a pelvic inclinometer to evaluate the pelvic inclination angle and an inclinometer to examine the lumbar angle.
Keywords: Polycystic Ovary Syndrome (PCOS), Hyperandrogenism, Ovulatory dysfunction, Insulin resistance, Hormonal imbalance, Androgen excess, Hirsutism, Infertility
INTRODUCTION: One of the most prevalent endocrine disorders, polycystic ovarian disease (PCOD), affects six to ten percent of women in the world who are of reproductive age. Hormonal imbalances, metabolic dysfunction, and genetic susceptibility combine intricately to cause a range of reproductive and metabolic illnesses 1.
One of the most prevalent endocrine system conditions affecting women of reproductive age is polycystic ovarian syndrome (PCOS), also known as hyperandrogenic an ovulation (HA) or Stein–Leventhal syndrome 2.
Infertility affects about 1 in 7 couples in the UK. It is more common in those who live with a partner later in life, have higher socioeconomic status, have higher levels of education, have higher occupational status, and, for those who already have children, become parents later in life 3. Recent studies have demonstrated that disorders of the gut microbiota (GM) are directly linked to the onset and progression of metabolic diseases, including insulin resistance, hyperandrogenism, chronic inflammation, and metabolic syndrome (diabetes, obesity), and may also play a role in the development of PCOS 4. Neuron-specific deletion of the androgen receptor (AR) was shown to prevent ovulatory failure and correct the increased adiposity caused by postnatal exposure to androgens in a preclinical model of PCOS. Therefore, one possible explanation in the pathophysiology of PCOS could be increased androgen signaling in the brain 5. Nonetheless, a prevalent misconception regarding GWAS is that they pinpoint certain genes. They only offer details about a genetic area (gene loci) that has a strong correlation with the characteristic. On the one hand, the detected gene loci may have a regulatory role for genes upstream or downstream, or they may be directly involved in gene function if they are found in or close to a gene. Therefore, GWAS-identified genetic loci offer suitable a priori candidate genes to study that are found inside these loci 6.
Obesity, hyperinsulinemia/insulin resistance, irregular menstruation, and oligo-/anovulation are the primary clinical signs of PCOS. Higher levels of androgen and estrogen but reduced levels of progesterone are the main hormonal abnormalities associated with PCOS. A number of factors have been linked to the development of PCOS, which may eventually result in female infertility due to poor follicle maturation and embryo implantation 7. Additionally, a higher incidence of metabolic problems such as insulin resistance (IR), glucose intolerance, type 2 diabetes mellitus (T2DM), dyslipidemia, and cardiovascular illnesses has been associated with PCOS. As a result, the impact of PCOS on women's health in general has received more attention. The origin and pathogenesis of PCOS remain unclear to this day 8. Many plants have shown promise in treating polycystic ovarian syndrome, including Saraca asoka, Moringa olifera, Asparagus racemosus, Cimicifuga racemose, and others 9.
Women with a genetic predisposition are more likely to develop PCOS, but environmental factors including obesity and sedentary lifestyles, as well as a diet heavy in unhealthy fats, can also accelerate the condition's emergence. Fifty percent of PCOS patients are obese or overweight. Many women with PCOS have been discovered to have insulin resistance, even if they are not obese. Additionally, insulin resistance and hyper-insulinemia are present in 40% to 50% of PCOS-affected women and 80% of obese PCOS-affected women, respectively 10. Menstrual abnormalities, hirsutism, and infertility due to hyperandrogenism and anovulation are clinical manifestations of PCOS in women. Although the exact cause of PCOS is still unknown, environmental and genetic factors have been linked to its development. Hyperinsulinemia and insulin resistance are linked to polycystic ovarian syndrome 11. What is known is that it depends on some ovarian tissue being destroyed, and in order for that to happen, the ovary needs to be given a specific amount of energy by a minimally intrusive method. Endocrine alterations following ovarian drilling appear to be controlled by the ovaries themselves, as suggested by Hendriks et al. (2007) 12.
Pro-inflammatory cytokines, chemokines, and oxidative stress indicators are elevated in chronic inflammation, which is a typical side effect of several metabolic disorders and is connected to IR. According to published studies, women with PCOS may have increased levels of inflammatory markers or their gene variants. While several studies reported TNF-α and IL-6 gene polymorphisms among PCOS women in relation to hyperandrogenic phenotypic features, Boulman et al. showed higher hs-CRP levels among insulin-resistant women with PCOS, comparable to that seen by Mazibrada et al. 13. Less research has been done on the environmental determinants of PCOS and its phenotype. While we know that obesity (and related increased sedentary lifestyle, poor nutrition, and overeating) exacerbates the metabolic complications of PCOS, there is little evidence that obesity itself causes the disorder to develop, nor is there clear evidence of significant differences in diet between women with and without PCOS. Other environmental factors that may determine the prevalence or phenotype of PCOS, altitude, latitude/longitude, climate, or topography 14.
Infertility, acne, excessive hair growth, and enlarged multicystic ovaries are among symptoms of PCOS in women. Researchers have postulated that insulin resistance plays a role in the development of PCOS and other chronic conditions like obesity, metabolic syndrome, cardiovascular disease, hypertension, and type 2 diabetes mellitus, though the exact cause is unknown (Dunaif, 1997; Steinberger & Daniels, 2003). According to research by Kahsar-Miller, Nixon, Boots, Go, and Azziz (2001), between 24% and 32% of women with PCOS had a mother or sister who had hyperandrogenism symptoms and insulin resistance 15.
It is frequently associated with elevated levels of two male hormones in the body. This hormone makes it more difficult for individuals to become pregnant and causes their body to skip menstruation cycles. PCOS-affected women produce more masculine hormones than usual. PCOS side effects manifest in a variety of unique ways. Some women will experience mild or modest adverse effects, while others will experience several severe negative effects. PCOS side symptoms include mood swings, depression, anxiety, and low self-esteem. Additionally, indications may change throughout different phases of a woman's life 16. On the other hand, additional research has demonstrated that when a female fetus is exposed to elevated levels of androgens from the mother, normal aromatization in the placenta, if maintained, does not cause PCOS. A genetic foundation for hyperandrogenism in PCOS was proposed by Legro et al. Candidate genes in the pathophysiology of PCOS include those involved in steroid production, particularly cytochrome P450. To determine their relationship to PCOS, these potential genes have been thoroughly investigated 17.
Other names for this syndrome are Schlerocystic Ovaries, Multicystic Ovaries, and Stein Leventhal Syndrome, which was coined by American gynecologists Michael L. Leventhal and Irving F. Stein, SR. Females between the ages of 18 and 44 are affected by this endocrine condition. It affects 5–15% of women worldwide. The ovary's operation and the control of the menstrual cycle, which preserves fertility, are both significantly impacted by hormone function. A persistent hormonal imbalance in females will disrupt ovarian function, resulting in the development of a cyst within the ovarian sac. On the other hand, females with PCOS had high levels of androgen, a masculine hormone 18. The disruption of the hypothalamic-pituitary axis, which leads to abnormal gonadotropin secretion by the hypothalamus and consequently elevated levels of luteinizing hormone (LH) and normal or low levels of follicle-stimulating hormone (FSH), is one of the many theories put forth to explain the pathogenesis of the syndrome 19. The Rotterdam 2003 criteria are currently acceptable for the diagnosis of PCOS, where two out of the following three criteria are satisfied: anovulation/oligoovulation, clinical and biochemical sign of hyperandrogenism and polycystic ovaries, after excluding other ae- tiologies such as congenital adrenal hyperplasia and androgen-secreting tumours. Insulin resistance (IR), hyperlipidemia, obesity, oxidative stress, type 2 diabetes mellitus (T2DM), and an elevated risk of cardiovascular disease (CVD) are among the metabolic effects of PCOS 20.
Recent research by our lab and others has demonstrated elevated androgen production in subcutaneous adipose tissue (SAT), which may be a factor in hyperandrogenism associated with PCOS. It is also known that adipose tissue plays a significant role in the overproduction of pro-inflammatory mediators, which leads to chronic inflammation in women with PCOS and other insulin-resistant diseases like obesity 21. Because P. acnes is so common, its function is unclear. Nonetheless, some acne strains may be more pro-inflammatory and linked to acne. Antibiotics used to treat acne seem to have anti-inflammatory benefits separate from their antimicrobial actions, notwithstanding the ongoing controversy over P. acnes. Because of this, broad-spectrum oral and topical antibiotics are the first-line treatment for acne, and these therapies must last at least three to six months 22. The body can get enough calcium from a well planned, well-balanced plant-based diet. People who don't eat plant-based meals high in calcium may be more susceptible to bone fractures and poor bone mineralization. The secret to healthy bones is a sufficient intake of calcium, which seems to be independent of dietary choices. 5 Tofu, mustard and turnip greens, bok choy, and kale are a few plant-based calcium sources 23.
Adolescent PCOS is still a significant clinical problem from both a diagnostic and therapeutic perspective. To restore ovulation, however, early PCOS diagnosis and treatment are essential. Changes in lifestyle, such as diet, exercise, and behavioral therapy, are the primary line of treatment for teenagers with PCOS 24. In order to answer the main question: Based on a meta-analysis of gold standard clamp studies, what is the degree of intrinsic IR in PCOS and the relative contribution of BMI to overall IR? Additionally, we sought to evaluate IR using other PCOS diagnostic criteria. In women with and without PCOS, our secondary goal was to examine important correlations between IR, BMI, SHBG, and other reproductive hormones (testosterone, LH, and FSH) and evaluate the possible function of SHBG as an IR marker 25.
Pathophysiology: Androgen excess, which affects 60% to 80% of PCOS patients, is a significant feature of the disorder. Hirsutism and hyperandrogenism are adverse effects of high androgen production. In fact, hyperandrogenism is the most common anomaly seen in PCOS, and it plays a major role in the aberrant hormones that lead to PCOS pathogenesis. One typical sign of hyperandrogenism is elevated blood levels of free testosterone 26. Early puberty is when PCOS first appears. The majority of pertinent data, however, has been gathered from adult female clinical trials where referral bias concentrates on examining the more severe phenotypes.
In-vitro and animal preclinical models complement clinical research and gain from alternative methods of studying this complicated condition. Neuroendocrine involvement in the etiology of PCOS is highlighted by recent clinical, experimental, and genetic findings 27.
The pathophysiology of PCOS has been explained by a number of ideas, including:
- Hyperinsulinemia and insulin resistance are caused by a specific abnormality in the action and secretion of insulin.
- An increased frequency and amplitude of the LH pulse due to a primary neuroendocrine abnormality.
- An increase in ovarian androgen production due to a malfunction in androgen synthesis.
A change in the metabolism of cortisol that leads to increased synthesis of adrenal androgen. However, it must be acknowledged that all of these are artificial statements that indicate the intimate relationship between the metabolic, ovarian, and pituitary circuits 28.
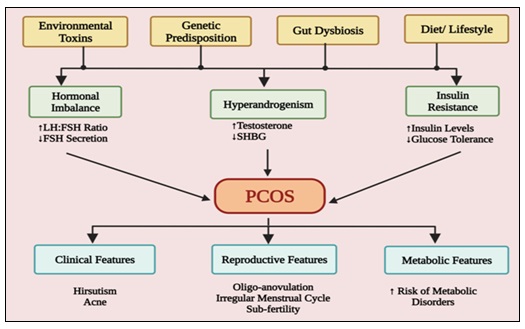
FIG. 1: THE SUGGESTED PATHOGENESIS AND CHARACTERISTICS OF PCOS ARE DEPICTED IN THIS SCHEMATIC FIGURE. THE ETIOLOGY OF PCOS AND THE SUBSEQUENT DEVELOPMENT OF CLINICAL, REPRODUCTIVE, AND METABOLIC CHARACTERISTICS IN PCOS PATIENTS ARE CAUSED BY RISK FACTORS SUCH AS ENVIRONMENTAL POLLUTANTS, GENETICS, GUT DYSBIOSIS, AND NUTRITION. FOLLICLE STIMULATING HORMONE (FSH), LUTEINIZING HORMONE (LH), AND SEX HORMONE BINDING GLOBULIN (SHBG)
The pathophysiology of polycystic ovarian syndrome (PCOS) includes innate ovarian dysfunction that is heavily impacted by extrinsic variables, including hyperinsulinemia and disruptions of the hypothalamic-pituitary-ovarian axis. Luteinizing hormone (LH) is hypersecreted as a result of increased gonadotrophin releasing hormone (GnRH) pulsatility, which affects ovarian androgen production as well as oocyte development. Gonadotrophin disorders are exacerbated by disrupted ovarian-pituitary and hypothalamus feedback. Both peripheral insulin resistance and aberrant pancreatic beta cell activity are secondary causes of hyperinsulinemia. PCOS is inherited, and a variety of genetic disorders seem to cause the syndrome's characteristics and explain the range of symptoms 29.
Harmonal Imbalance and Hyperandrogenism: The prevalent endocrine condition known as polycystic ovarian syndrome (PCOS) is typified by metabolic dysfunction and hormonal imbalance. The hypothalamic-pituitary-ovarian (HPO) axis's dysregulation is a key characteristic of PCOS. Luteinizing hormone (LH) is higher in comparison to follicle-stimulating hormone (FSH) due to increased pulsatile production of gonadotropin-releasing hormone (GnRH). This imbalance hinders normal follicular development and ovulation by stimulating ovarian theca cells and producing excess androgen 30. PCOS is characterized by hyperandrogenism, which can manifest clinically as hirsutism, acne, and androgenic alopecia. Elevated levels of testosterone, androstenedione, and dehydroepiandrosterone sulfate (DHEAS) are biochemical indicators. Excess androgens are mostly produced by the ovaries, though the adrenal glands may also play a role. By raising insulin levels, which in turn increase androgen production in the ovaries and decrease hepatic synthesis of sex hormone-binding globulin (SHBG), insulin resistance, which is often linked to PCOS, aggravates hyperandrogenism. Clinical symptoms worsen when SHBG levels are lower because free androgens are more bioavailable 31. Furthermore, tiny, stalled follicles accumulate as a result of poor folliculogenesis; these follicles are frequently visible on ultrasonography as "polycystic" ovaries. Anovulation and irregular menstrual periods are exacerbated by this. Long-term issues like type 2 diabetes, heart disease, and endometrial hyperplasia are also made more likely by persistent hormonal imbalance 32. The pathophysiology of PCOS is primarily caused by the interaction of androgen excess, insulin resistance, and neuroendocrine dysfunction, which results in a self-sustaining loop. In order to improve reproductive results and restore endocrine balance, effective care frequently targets these processes using hormonal therapies, insulin-sensitizing medications, and lifestyle modifications 33.
Insulin Resistance and Metabolic Dysfunction: Insulin resistance is a central feature of Polycystic Ovary Syndrome and plays a key role in its metabolic and reproductive manifestations. In many individuals with PCOS, peripheral tissues such as muscle and adipose exhibit reduced sensitivity to insulin, leading to compensatory hyperinsulinemia. This excess insulin not only disrupts glucose homeostasis but also exacerbates ovarian androgen production by stimulating theca cells and suppressing hepatic synthesis of sex hormone–binding globulin (SHBG). As a result, circulating free androgens increase, contributing to clinical symptoms such as hirsutism, acne, and ovulatory dysfunction 33. Beyond insulin resistance, metabolic dysfunction in PCOS includes an elevated risk of impaired glucose tolerance, type 2 diabetes, dyslipidemia, and central obesity; altered adipokine secretion and chronic low-grade inflammation exacerbate insulin signaling pathways; and oxidative stress and mitochondrial dysfunction have been linked to the pathophysiology, indicating that PCOS is a complex metabolic condition rather than just a reproductive disorder. Since long-term metabolic problems have a major impact on cardiovascular health, understanding insulin resistance in PCOS is essential for early intervention. Effective management requires a thorough strategy that takes into account both endocrine and metabolic factors 19. Obesity is a contributing factor to the varying prevalence and severity of insulin resistance in PCOS. However, intrinsic insulin signaling abnormalities may be present in even thin PCOS patients, suggesting a genetic or molecular basis. Insulin resistance is frequently addressed by management techniques that involve lifestyle changes like diet, exercise, and weight loss. Metformin is one example of a pharmaceutical treatment that increases insulin sensitivity and may help control metabolic parameters and menstrual periods 34.
Chronic Inflammation and Oxidative Stress: It is becoming better acknowledged that oxidative stress and chronic inflammation play a major role in the pathophysiology of polycystic ovary syndrome. Low-grade chronic inflammation, which is typified by increased levels of inflammatory markers such C-reactive protein (CRP), interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-α), is frequently seen in PCOS patients. It is believed that excess adipose tissue, especially visceral fat, which actively secretes pro-inflammatory cytokines, is the source of an inflammatory milieu. These mediators increase insulin resistance and contribute to the metabolic abnormalities frequently seen in PCOS by interfering with insulin signaling pathways. Oxidative stress and chronic inflammation interact to create a vicious cycle. While oxidative stress triggers other inflammatory signaling pathways including nuclear factor-kappa β (NF-κB), inflammatory activities increase the generation of ROS. This reciprocal link increases the likelihood of long-term consequences including type 2 diabetes and cardiovascular disease by amplifying metabolic and endocrine problems 35. By causing an imbalance between the body's antioxidant defense systems and reactive oxygen species (ROS), oxidative stress makes this situation worse. Chronic inflammation, hyperglycemia, and mitochondrial dysfunction may all contribute to increased ROS generation in PCOS. Increased oxidative stress can harm cellular lipids, proteins, and DNA, which can hinder normal follicular development and ovarian function. The two main reproductive characteristics of PCOS, anovulation and low oocyte quality, are exacerbated by this disturbance. Lifestyle changes like losing weight, eating a balanced diet, and engaging in regular exercise are management techniques that address oxidative stress and inflammation. Oxidative damage may be lessened by diets high in antioxidants, such as omega-3 fatty acids, polyphenols, and vitamins C and E. Insulin-sensitizing medications and anti-inflammatory therapies are examples of pharmacological approaches that have the potential to improve clinical outcomes. Comprehensive PCOS management requires addressing these fundamental systems 36.
Genetic and Environmental Factors: Increasing evidences over many years point to familial aggregation of women with PCOS, hyperandrogenism and metabolic alterations. The model of inheritance of PCOS has not yet been defined. Some researchers have postulated autosomal dominant transmission linked to a single genetic defect, but most authors define PCOS as a polygenic pathology. It is also possible that a particular gene in a given family may have a predominant effect, influencing the phenotypic manifestations of the syndrome. The primary candidate genes are those that code for elements related to androgen synthesis, transport, regulation, and effects 37. Genome-wide association studies carried out across several populations have gradually shed light on the genetic architecture of polycystic ovarian syndrome. More than twenty susceptibility loci have been found thus far; the strongest signals correspond to genes related to follicular development, insulin signaling, androgen production, and gonadotropin control. Through alternate splicing methods, the DENND1A gene on chromosome 9 appears consistently across ethnic groups and appears to be responsible for the overproduction of androgen in theca cells. Polymorphisms in INSR and IRS1 link the condition to more general metabolic abnormalities, while variations close to the LHCGR gene affect luteinizing hormone receptor sensitivity. Strong genetic programming is clearly implied by twin experiments, which estimate heritability at 70% or more. The problem is that heredity is not fate 38.
Environmental variables are becoming increasingly important, as seen by the rise in PCOS prevalence in societies where the gene pool has remained relatively steady. In those who are at risk, the onset of PCOS is associated with the development of obesity. Positive energy balance is typical in developed nations because of the low daily energy expenditure and plentiful, reasonably priced food supply. Even said, this perspective is overly basic, and it's possible that other environmental factors such as exposure to environmental pollutants may also be at play 39.
Role of Herbal Medicine in PCOS Management: In the treatment of Polycystic Ovary Syndrome (PCOS), a complicated endocrine condition marked by hyperandrogenism, ovulatory dysfunction, and insulin resistance, herbal medicine has drawn interest as a supplemental strategy. Numerous herbal treatments focus on important pathophysiology elements of PCOS, such as inflammation, metabolic dysfunction, and hormonal imbalance 40. Numerous herbs have shown promise. By modulating the hypothalamic-pituitary-ovarian axis and raising progesterone levels, Vitex agnus-castus, or chasteberry, is frequently used to control menstrual cycles. It has been demonstrated that Cinnamomum verum, or cinnamon, increases insulin sensitivity, which is important because insulin resistance is a significant cause of PCOS. In a similar vein, fenugreek, or Trigonella foenum-graecum, may help lower blood sugar and enhance lipid profiles 41. Herbs that are anti-androgenic, including licorice (Glycyrrhiza glabra), can reduce testosterone levels, which may lessen symptoms like acne and hirsutism. The adaptogen Withania somnifera, often known as ashwagandha, may help regulate cortisol and stress levels, so indirectly promoting hormonal balance. Furthermore, Curcuma longa, or turmeric, has antioxidant and anti-inflammatory qualities that may reduce PCOS-related chronic inflammation 42.
Herbal medicine should be used with caution, despite encouraging results. The effectiveness and safety of herbal products can be impacted by variations in dosage, preparation, and quality. Interactions with traditional drugs also need to be taken into account. Therefore, it is recommended to take herbal remedies under the supervision of a specialist as part of an integrative treatment plan that also include dietary and activity changes. In conclusion, by treating hormonal, metabolic, and inflammatory pathways, herbal medicine provides supporting advantages in the management of PCOS. To create standardized procedures and verify long-term safety and efficacy, however, more thorough clinical trials are required 43.
Historical and Traditional Perspectives: Long before it was formally classified in modern medicine, Polycystic Ovary Syndrome (PCOS) was understood through both traditional healing systems and historical medical frameworks. PCOS is acknowledged in modern biomedicine as an endocrine and metabolic condition marked by polycystic ovarian morphology, ovulatory dysfunction, and hyperandrogenism.
However, historical and traditional viewpoints offer important insights into how PCOS-like symptoms were perceived and treated 44. PCOS-related symptoms were frequently linked to ailments like Yonivyapad (gynecological diseases) and Artava Kshaya (menstrual irregularity) in ancient Ayurvedic writings. According to Ayurveda, these disorders are caused by imbalances in the doshas, especially Kapha and Vata, which result in poor metabolism (Agni) and toxin buildup (Ama). Herbal remedies (such Ashoka and Shatavari), diet control, detoxification (Panchakarma), and lifestyle changes like yoga and meditation were among the ancient forms of treatment 45. In a similar vein, dysfunction in organ systems, especially the kidneys, liver, and spleen, is how Traditional Chinese Medicine (TCM) explains PCOS symptoms. Hormonal imbalance and cyst formation are frequently explained by ideas like "phlegm-dampness accumulation" and "Qi stagnation." Acupuncture, herbal remedies (such Cang Fu Dao Tan Tang), and food therapy are some of the TCM treatments used to improve reproductive health and restore equilibrium.
PCOS symptoms are associated with imbalances in physiological humors, particularly excess Balgham (phlegm), according to Greco-Arab (Unani) medicine. Herbal remedies, dietary changes, and regimental therapy are used to address humoral imbalance. Despite the differences in nomenclature and conceptual frameworks between these traditional systems, metabolic disorders, lifestyle variables, and systemic imbalance are commonalities. In order to manage PCOS, modern research is increasingly investigating integrative techniques, acknowledging that traditional practices particularly those that focus on food, stress, and physical activity may supplement biological treatments 46.
Advantages of Plant-Based Therapeutics: Because of their multi-targeted effects, affordability, and generally good safety profiles, plant-based therapies have drawn more interest in the treatment of Polycystic Ovary Syndrome (PCOS). Insulin resistance, hyperandrogenism, persistent inflammation, and ovulatory dysfunction are the hallmarks of PCOS, a complicated endocrine condition. Compounds produced from plants and herbs can affect multiple pathways at once, which makes them especially well-suited for holistic treatment. Standardization, dose control, and thorough clinical validation are still difficulties in spite of these benefits 47. Their capacity to increase insulin sensitivity is one of their main benefits. Since insulin resistance is a key component of PCOS, plants like Trigonella foenum-graecum (fenugreek) and Cinnamomum verum (cinnamon) have shown promise in reducing blood glucose levels and improving insulin signaling. In several trials, Berberis aristata, a source of berberine, has demonstrated results similar to those of traditional insulin-sensitizing medications 48. The control of hormone imbalance is an additional advantage. Herbs like Paeonia lactiflora (white peony) and Glycyrrhiza glabra (licorice) may help lower androgen levels, relieving symptoms like acne and hirsutism. Additionally, adaptogenic botanicals like ashwagandha (Withania somnifera) help regulate cortisol and reduce stress, which indirectly promotes hormonal balance. Additionally, plant-based therapies are typically more widely available and socially acceptable, especially in areas with a high prevalence of traditional medical systems like Ayurveda. They can improve long-term adherence and results when combined with lifestyle changes like diet and exercise 49. The efficacy of plant-based medicines is further enhanced by their anti-inflammatory and antioxidant characteristics. PCOS patients frequently have chronic low-grade inflammation, and plants high in polyphenols, such green tea (Camellia sinensis), assist lower oxidative stress and enhance metabolic results 50.
Safety and Toxicological Considerations: The multifactorial endocrine condition known as polycystic ovarian syndrome (PCOS) necessitates long-term treatment, which frequently entails dietary, medication, and lifestyle changes. Because of the metabolic vulnerabilities linked to PCOS and the long-term exposure to drugs and supplements, safety and toxicological considerations are crucial 51. Insulin sensitizers (like metformin), oral contraceptives, anti-androgens, and ovulation-inducing drugs are frequently used in pharmacotherapy. These medications can be dangerous even if they are usually effective. Particularly in those with renal impairment, metformin may result in gastrointestinal issues and, in rare cases, lactic acidosis.
Combined oral contraceptives are linked to a higher risk of thromboembolism, particularly in smokers and obese women, who are already more likely to develop PCOS. Anti-androgens like spironolactone need to be closely watched because they can cause hyperkalemia 52. From a toxicological standpoint, long-term drug usage requires assessment of cumulative exposure and organ-specific damage, especially renal and hepatic function. Concerns about purity, dosage uniformity, and possible drug interactions are also raised by the growing usage of herbal supplements (such as inositol, cinnamon, and herbal mixes). Many of these supplements have not undergone thorough toxicological testing 53. Toxicants in the environment also have an impact. Insulin resistance and hormonal imbalance in PCOS have been linked to endocrine-disrupting chemicals (EDCs), including phthalates, bisphenol A (BPA), and persistent organic pollutants. Long-term low-dose exposure may exacerbate the severity of the illness and make treatment more difficult 54. Although helpful, nutritional interventions must be balanced to prevent excesses or deficits, especially with restrictive diets. Drug pharmacokinetics are changed by obesity, which is prevalent in PCOS and may have an impact on toxicity and efficacy. In conclusion, medication efficacy and safety must be carefully balanced when controlling PCOS. To reduce toxicological hazards, tailored treatment, routine monitoring, and knowledge of supplementary and ambient exposures are crucial 55.
Mechanisms of Action of Plant-Based Interventions: Due in large part to their multi-targeted mechanisms of action, plant-based therapies have drawn interest as supplemental methods for treating Polycystic Ovary Syndrome (PCOS). These treatments frequently have positive effects by modifying oxidative stress, insulin resistance, androgen levels, and inflammation 56. Insulin resistance is a key component of PCOS. Numerous substances produced from plants, including flavonoids and polyphenols, increase glucose absorption and activate signaling pathways including AMP-activated protein kinase (AMPK) to improve insulin sensitivity. For instance, substances in fenugreek and cinnamon assist control blood sugar levels and lower hyperinsulinemia, which in turn reduces the production of androgens in the ovaries 57.
Another characteristic of PCOS is hyperandrogenism. Some herbs have been shown to have anti-androgenic qualities, including licorice root and spearmint. These may improve symptoms like hirsutism and acne by lowering circulating testosterone levels or blocking enzymes like 5-alpha reductase. Furthermore, by attaching to estrogen receptors and altering endocrine function, phytoestrogens present in flaxseed and soy may aid in maintaining hormonal balance. Both ovulatory function and normal menstruation may benefit from this 58. Overall, by focusing on several PCOS-related pathways, plant-based medicines provide a comprehensive approach and are therefore promising supplements to traditional treatments 59.
Anti-androgenic Effects: Hyperandrogenism, ovulatory dysfunction, and polycystic ovarian morphology are the hallmarks of PCOS, a prevalent endocrine condition. In order to treat clinical symptoms including hirsutism, acne, and androgenic alopecia, anti-androgenic medication is essential. These treatments work by either inhibiting androgen receptors in the target tissue or decreasing androgen synthesis. The first-line pharmacological treatment for hyperandrogenism in PCOS is thought to be combined oral contraceptives (COCs). They reduce the generation of androgens in the ovaries by suppressing the secretion of luteinizing hormone (LH). Furthermore, the estrogen component lowers free circulating testosterone via raising sex hormone-binding globulin (SHBG). Drospirenone and cyproterone acetate, two progestins found in COCs, have inherent anti-androgenic qualities that increase their therapeutic impact. Finasteride, flutamide, and spironolactone are additional anti-androgenic medications. Spironolactone reduces the conversion of testosterone to its more potent form, dihydrotestosterone (DHT), by acting as an androgen receptor antagonist and inhibiting 5α-reductase activity. The use of flutamide, a nonsteroidal anti-androgen that directly blocks androgen receptors, is restricted because of the possibility of hepatotoxicity. By reducing DHT levels, finasteride, a 5α-reductase inhibitor, is very useful in treating hirsutism. Hyperandrogenism is also influenced by insulin resistance, a major characteristic of PCOS. By increasing insulin sensitivity and reducing ovarian androgen production, insulin-sensitizing medications such as metformin indirectly lower androgen levels. Overall, by addressing both the hormonal imbalance and its clinical effects, anti-androgenic treatments greatly enhance the quality of life for women with PCOS. Treatment should, however, be customized, taking into account any potential adverse effects and contraindications 60.
Insulin-Sensitizing Properties: One of the main characteristics of Polycystic Ovary Syndrome (PCOS) and a major factor in its pathogenesis is insulin resistance. It contributes to metabolic and reproductive problems and is found in both lean and obese women with PCOS. By activating ovarian theca cells and inhibiting the hepatic synthesis of sex hormone-binding globulin (SHBG), elevated insulin levels boost androgen production and raise free testosterone levels. Menstrual abnormalities, acne, and hirsutism are all made worse by this hormonal imbalance. Additionally, insulin resistance raises the risk of type 2 diabetes, decreased glucose tolerance, and cardiovascular problems. Thus, one of the main therapeutic goals in the treatment of PCOS is to increase insulin sensitivity. To treat this metabolic inefficiency and enhance overall clinical results, both pharmaceutical and non-pharmacological approaches are used 61. The most often prescribed insulin-sensitizing medication for PCOS is metformin. It lowers circulating insulin levels by enhancing peripheral glucose absorption and decreasing hepatic glucose synthesis. This drop in insulin may help some women regain their ovulatory cycles by reducing the generation of ovarian androgens. Furthermore, dietary changes, weight reduction, and regular exercise are examples of lifestyle therapies that greatly increase insulin sensitivity and boost the efficacy of medication. Thiazolidinediones may also be utilized in some circumstances, albeit its use is restricted due to possible adverse effects. In general, treating insulin resistance enhances metabolic health and benefits reproductive function in PCOS-affected women 62.
Anti-inflammatory and Antioxidant Activities: It is becoming more well acknowledged that oxidative stress and chronic low-grade inflammation play a significant role in the pathogenesis of PCOS. Inflammatory indicators such C-reactive protein (CRP), interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-α) are frequently high in women with PCOS. These inflammatory mediators are intimately associated with hyperandrogenism and insulin resistance, creating a vicious cycle that worsens reproductive and metabolic problems. Furthermore, an imbalance between antioxidant defenses and reactive oxygen species (ROS) can lead to oxidative stress, which can increase hormonal imbalances, alter follicular growth, and impair ovarian function. As a result, addressing oxidative stress and inflammation has emerged as a key therapeutic strategy for PCOS treatment 63. Numerous dietary and pharmacological treatments have shown anti-inflammatory and antioxidant benefits in PCOS. In addition to increasing insulin sensitivity, medications like metformin also lower oxidative stress and inflammatory markers. Additionally, substances like flavonoids and polyphenols, as well as dietary antioxidants like vitamins C and E, aid in the neutralization of ROS and enhance cellular activity. Changes in lifestyle, especially consistent exercise and a well-balanced diet full of fruits, vegetables, and whole grains, improve antioxidant capacity and lower systemic inflammation. Additionally, there is growing evidence that supplementation like omega-3 fatty acids can reduce inflammatory cytokines. In general, treatments that address oxidative stress and inflammation have a major positive impact on the metabolic and reproductive outcomes of PCOS-affected women 64.
Modulation of Ovarian Function: A key objective in the treatment of Polycystic Ovary Syndrome, a disorder marked by abnormal folliculogenesis and persistent anovulation, is to modify ovarian function. Hyperinsulinemia and elevated luteinizing hormone (LH) release in PCOS cause ovarian theca cells to overproduce androgens, which hinder normal follicular development. Menstrual abnormalities and infertility come from the accumulation of numerous little follicles without ovulation. Correcting hormonal imbalances, lowering androgen levels, and encouraging follicular development and ovulation are the main therapeutic approaches used to restore normal ovarian function 65. Pharmacological treatments are frequently used to control ovarian activity and induce ovulation. Clomiphene citrate, which enhances follicle-stimulating hormone (FSH) output and accelerates follicular development by blocking estrogen receptors in the hypothalamus, is frequently the first-line medication for ovulation induction. Letrozole, which decreases estrogen production and increases FSH release, is another frequently used medication that has been demonstrated in certain trials to improve ovulation and live birth rates. Additionally, by lowering insulin and androgen levels, insulin-sensitizing medications like metformin can indirectly enhance ovarian function. Gonadotropin treatment or assisted reproductive technologies may be taken into consideration in cases of resistance. Restoring ovulatory cycles also heavily depends on lifestyle changes, such as exercise and weight control. Overall, ovarian function is effectively modulated and reproductive outcomes are improved in women with PCOS when pharmaceutical and lifestyle interventions are combined 66.
Key Medicinal Plants Used in PCOS Treatment: Due to its ability to target several pathophysiological pathways, including insulin resistance, hyperandrogenism, and chronic inflammation, herbal medicine has drawn more interest as an adjunctive treatment for Polycystic Ovary Syndrome. Numerous therapeutic plants have shown encouraging results in enhancing PCOS-affected women's metabolic and reproductive outcomes. Among these, the insulin-sensitizing qualities of Cinnamomum verum, or cinnamon, have been extensively researched. It increases insulin signaling and glucose absorption, which may help control menstrual periods and lower androgen levels. Similarly, it has been demonstrated that the bioactive substances of Trigonella foenum-graecum enhance insulin resistance and boost ovarian function 67. Glycyrrhiza glabra is another significant medicinal herb with anti-androgenic qualities. It can alleviate symptoms like hirsutism and lower testosterone levels. When taken as herbal tea, Mentha spicata has also been shown to have anti-androgenic properties, especially in lowering levels of free testosterone. Furthermore, Withania somnifera has adaptogenic and anti-inflammatory qualities that may lessen hormonal imbalances brought on by stress and enhance insulin sensitivity. The antioxidant and endocrine-modulating properties of these plants are often attributed to the presence of polyphenols, flavonoids, and other phytochemicals. Despite encouraging results, there is still little and inconsistent clinical evidence to support the use of medicinal herbs for PCOS. Potential herb-drug interactions, long-term safety, and dosage standardization must all be carefully taken into account. Instead of being utilized as stand-alone treatments, herbal remedies should be used in conjunction with conventional medicines under physician supervision. By focusing on important underlying mechanisms, medicinal plants provide a comprehensive approach to PCOS management 68.
Withania somnifera (Ashwagandha): In traditional Ayurvedic medicine, Withania somnifera, also known as ashwagandha, is a well-known medicinal herb prized for its antioxidant, adaptogenic, and anti-inflammatory qualities. Ashwagandha's ability to regulate hormone balance and enhance metabolic health has drawn attention in relation to Polycystic Ovary Syndrome. Chronic stress, high cortisol, insulin resistance, and hyperandrogenism are frequently linked to PCOS. By lowering cortisol levels brought on by stress, ashwagandha helps control the hypothalamic-pituitary-adrenal (HPA) axis, which may tangentially enhance ovarian function and menstrual regularity 69. Ashwagandha has also been demonstrated to improve insulin sensitivity and lower inflammation, two important aspects of the pathogenesis of PCOS. Its bioactive substances, such as withanolides, can lower oxidative stress and enhance glucose metabolism. These actions could help reduce the amount of testosterone in the blood and ease symptoms like infertility and irregular cycles. Ashwagandha is regarded as a promising supplementary therapy for PCOS control, despite the fact that clinical evidence is still being gathered. It should, however, be used carefully and under a doctor's supervision, particularly when taking it alongside prescription drugs 70.
Cinnamomum verum (Cinnamon): Because of its insulin-sensitizing and metabolic properties, Cinnamomum verum, or cinnamon, has been extensively researched for its possible medicinal function in treating Polycystic Ovary Syndrome (PCOS). One of the main characteristics of PCOS is insulin resistance, which contributes to ovulatory failure and hyperandrogenism.
Bioactive substances included in cinnamon, such as polyphenols, promote peripheral tissue glucose absorption and insulin receptor function. Cinnamon may indirectly lower ovarian androgen production and aid in the restoration of hormonal balance by lowering circulating insulin levels 71. Supplementing with cinnamon may enhance ovulation and menstrual cyclist in women with PCOS, according to clinical research. Additionally, it has been linked to lower fasting blood glucose and cholesterol levels, which improves metabolic management. Furthermore, cinnamon has anti-inflammatory and antioxidant qualities that may help lower oxidative stress and persistent low-grade inflammation, which are frequently seen in PCOS patients. It is a promising supplemental therapy because of these combined benefits. Despite these advantages, more extensive and prolonged clinical trials are required to determine uniform dosages and validate its safety and effectiveness. Instead of being utilized as a stand-alone treatment, cinnamon should be used in conjunction with traditional therapy and lifestyle changes 72.
Trigonella foenum-graecum (Fenugreek): Chronic metabolic dysfunction, hyperandrogenism, and insulin resistance are frequently linked to polycystic ovary syndrome (PCOS). Because of its high concentration of soluble fiber (galactomannan), steroidal saponins (diosgenin), and alkaloids, Trigonella foenum-graecum (fenugreek) has been extensively researched as a plant-based intervention for enhancing these characteristics 73. Enhancing insulin sensitivity is one of fenugreek's main effects on PCOS. While bioactive substances increase insulin receptor activation and glucose uptake in peripheral tissues, the high fiber content slows the absorption of carbohydrates and lowers postprandial glucose levels. This aids in reducing compensatory hyperinsulinemia, a major cause of increased testosterone in the ovaries 74.
Additionally, fenugreek's antioxidant qualities help lower oxidative stress, which is linked to follicular dysfunction and anovulation, and it may have indirect anti-androgenic effects by lowering insulin levels, which in turn reduces luteinizing hormone (LH)-stimulated androgen production in ovarian theca cells 75. Fenugreek supplementation has been proven in clinical research to enhance metabolic parameters, ovarian morphology, and menstrual regularity in women with PCOS; however, the effects vary based on formulation and dose. Fenugreek is a promising adjuvant in the treatment of PCOS because it acts through several routes, including metabolic, hormonal, and antioxidant 76.
Glycyrrhiza glabra (Licorice): Licorice, or Glycyrrhiza glabra, is a medicinal plant that is frequently utilized in ancient medical systems like Ayurveda and ancient Chinese Medicine. It has drawn interest due to its possible use in the treatment of Polycystic Ovary Syndrome (PCOS), a complicated endocrine condition marked by irregular ovulation, insulin resistance, and hyperandrogenism 77.
Glycyrrhizin, flavonoids, and phytoestrogens are among the bioactive substances found in licorice that support its medicinal properties. Its anti-androgenic impact is one of its most significant effects in PCOS. According to studies, licorice can lower serum testosterone levels by blocking androgen synthesis-related enzymes such 17 β-hydroxysteroid dehydrogenase and 17, 20-lyase. Acne and hirsutism symptoms may be lessened by this decrease. Additionally, licorice has insulin-sensitizing qualities, which are advantageous because insulin resistance is a major characteristic of PCOS. Licorice may indirectly lower ovarian androgen production and promote metabolic balance by increasing insulin sensitivity. Its antioxidant and anti-inflammatory properties may also aid in combating the persistent low-grade inflammation that PCOS patients frequently experience 78. When used in conjunction with other therapies, licorice may help maintain hormonal balance. For instance, it has been investigated in conjunction with drugs like spironolactone, where it may increase anti-androgen benefits while perhaps lowering adverse effects like hyperkalemia 79. But even with these encouraging advantages, licorice needs to be handled carefully. Because of its mineralocorticoid activity, excessive or prolonged use can cause negative effects such hypertension, hypokalemia, and fluid retention. Clinical supervision is therefore advised, particularly for long-term use. In conclusion, Glycyrrhiza glabra's anti-androgenic, metabolic, and anti-inflammatory qualities make it a promising adjunctive treatment for PCOS.
To determine its safety, ideal dosage, and long-term effectiveness, however, additional extensive clinical trials are required 80.
Mentha spicata (Spearmint): Spearmint, or Mentha spicata, is a culinary and medical herb that has gained popularity due to its possible advantages in treating PCOS. Hyperandrogenism, irregular menstruation, and metabolic problems are characteristics of PCOS, an endocrine condition. The anti-androgenic qualities of spearmint, which may help reduce some of these symptoms, have been the main focus of research 81.
Reducing circulating androgen levels is one of the main ways spearmint may help PCOS patients. According to clinical research, drinking spearmint tea can dramatically lower free testosterone levels while improving the balance of luteinizing hormone (LH) and follicle-stimulating hormone (FSH). This hormonal regulation may help alleviate PCOS symptoms including acne and hirsutism (excess body and face hair) 82. Because of its high concentration of phenolic components including flavonoids and rosmarinic acid, spearmint also has anti-inflammatory and antioxidant qualities. These characteristics are important since PCOS is frequently linked to oxidative stress and chronic low-grade inflammation. Spearmint may promote ovarian function and general endocrine balance by lowering oxidative damage 83. Furthermore, spearmint may have a slight insulin-sensitizing impact that could help manage insulin resistance, a key component of PCOS. Menstrual periods and ovarian androgen production may be better regulated with increased insulin sensitivity. Despite their small size, human studies yield encouraging results. For example, daily use of spearmint tea over a 30-day period has been shown in randomized controlled studies to reduce androgen levels and improve hirsutism subjectively. Larger, longer-term studies are required to validate these conclusions, though, as the data is still developing. When taken in moderation, as in tea, spearmint is generally regarded as safe. However, rather than taking the place of traditional medical care, it should be taken as a supplemental therapy 84.
Aloe vera: The potential benefits of aloe vera in treating Polycystic Ovary Syndrome, a hormonal disorder marked by irregular menstrual periods, insulin resistance, and high androgen levels, have been investigated. Vitamins, enzymes, polysaccharides, and antioxidants are among the bioactive substances found in aloe vera that may assist enhance hormonal and metabolic balance 85. Aloe vera gel may improve insulin sensitivity, which is crucial in PCOS because insulin resistance is a major factor, according to research. Better insulin function can assist control menstrual periods and ovulation by indirectly lowering testosterone production. Aloe vera's antioxidant and anti-inflammatory qualities may also promote ovarian health and lessen oxidative stress linked to PCOS 86. Aloe vera supplementation has been demonstrated to restore normal ovarian function and steroid balance in animal trials. However, there are still few human investigations, and additional clinical trials are required to verify its safety and effectiveness. Although aloe vera is often taken as juice or gel, long-term use and dose should be carefully considered. In conclusion, aloe vera may help control PCOS, especially with regard to metabolic issues, but it shouldn't take the place of medical care. Before using, it is advised to speak with a healthcare provider 87.
Camellia sinensis (Green Tea): Green tea, or Camellia sinensis, is rich in bioactive compounds, especially catechins like epigallocatechin gallate (EGCG), which have potent anti-inflammatory and antioxidant qualities. Green tea has gained attention for its potential role in managing Polycystic Ovary Syndrome, a condition linked to hormonal imbalance, insulin resistance, and metabolic disturbances 88. According to studies, green tea may help with one of the main underlying causes of PCOS by enhancing insulin sensitivity and glucose metabolism. It may also help lower androgen levels by lowering insulin resistance, which would alleviate symptoms like irregular menstruation and excessive hair growth. Green tea has also been associated with modest weight loss and decreased body fat, which can help women with PCOS even more because obesity frequently makes the problem worse 89. Regular green tea drinking may help control ovarian function and enhance lipid profiles, according to certain clinical and experimental research. Additionally, its antioxidant properties aid in lowering oxidative stress, which is higher in PCOS patients. Although these results are encouraging, more extensive human research is required to validate long-term advantages and the ideal dosage. In addition to medical care and lifestyle changes, green tea can be used as a supportive therapy 90.
Other Emerging Herbal Candidates: Because of their impact on insulin resistance, hormonal balance, and inflammation, a number of new herbal candidates are being investigated for their potential benefits in controlling Polycystic Ovary Syndrome. Cinnamon, or Cinnamomum verum, has showed potential in controlling menstrual cycles and enhancing insulin sensitivity. Clinical research indicates that supplementing with cinnamon may improve glucose metabolism and help women with PCOS regain ovulatory function 91. Another herb with anti-androgenic qualities is Glycyrrhiza glabra, or licorice. It might help lower testosterone levels, which would alleviate symptoms like acne and hirsutism. Similarly, lignans and omega-3 fatty acids found in Linum usitatissimum (flaxseed) may help reduce androgen levels and enhance lipid profiles 92. Fenugreek, or Trigonella foenum-graecum, has also drawn notice for its capacity to promote ovarian health and its insulin-sensitizing properties. According to certain research, fenugreek seed extracts might lessen the size of ovarian cysts and increase menstruation regularity 93. The majority of the data for these herbal choices comes from limited clinical trials or experimental investigations, despite their optimistic outcomes. To determine their safety, effectiveness, and ideal dosages, more extensive research is therefore required. These herbs can be used in addition to traditional medicines and lifestyle changes as complementary therapies 94.
Polyherbal Formulations and Synergistic Effects: Because they may have synergistic effects on hormonal, metabolic, and inflammatory pathways, polyherbal formulations which include several medicinal plants are being investigated more and more for the treatment of polycystic ovary syndrome. Polyherbal treatments, in contrast to single-herb therapy, address several elements of PCOS at once, including oxidative stress, hyperandrogenism, and insulin resistance 95. For example, traditional medical systems like Ayurveda frequently employ formulations that combine Withania somnifera, Tinospora cordifolia, and Emblica officinalis. Together, these herbs have antioxidant, anti-inflammatory, and adaptogenic qualities that may help control endocrine function and enhance ovarian health. In a similar vein, mixtures of Cinnamomum verum and Trigonella foenum-graecum may improve insulin sensitivity more successfully than individual ingredients 96. The idea of synergy suggests that the total therapeutic benefit of herbs is more than the sum of their individual benefits. This could enable more extensive therapeutic coverage, lower dosages, and fewer adverse effects. Preliminary clinical and experimental research indicates that using polyherbs can enhance glucose metabolism, lipid profile, and menstrual regularity. However, there is still no scientific validation, and uniformity is hampered by formulation variability. To verify safety, effectiveness, and ideal combinations, more thorough clinical trials are required 97.
Concept of Polyherbal Therapy: In order to obtain increased treatment efficacy, especially in complicated illnesses like Polycystic Ovary Syndrome, the notion of polyherbal therapy entails the mixing of several medicinal plants. Due to the multifactorial nature of PCOS, which includes insulin resistance, oxidative stress, inflammation, and hormonal imbalance, a multi-targeted treatment strategy is frequently thought to be advantageous 98. The concept of synergy, in which various herbs function through complementary processes, is the foundation for the creation of polyherbal compositions. For instance, Asparagus racemosus promotes hormonal balance and reproductive health, Gymnema sylvestre helps glucose metabolism, and Withania somnifera may help lower stress and control cortisol levels. When combined, these herbs can treat several PCOS underlying problems at once 99. Additionally, polyherbal therapy may minimize negative effects while increasing overall efficacy by lowering the necessary dosage of particular herbs. Furthermore, a variety of phytochemicals, including flavonoids, alkaloids, and saponins, have anti-inflammatory and antioxidant properties that are essential for PCOS management. Despite its benefits, there are also issues such inconsistent composition, lack of standardization, and scant large-scale clinical evidence. As a result, even if polyherbal therapy has potential as a supplemental strategy, it should be applied carefully and under a doctor's supervision 100.
Evidence Supporting Synergism: Research demonstrating synergism in the treatment of Polycystic Ovary Syndrome emphasizes the benefit of combining several herbal remedies to address its intricate pathophysiology. Because PCOS is caused by a number of interrelated variables, including oxidative stress, insulin resistance, hyperandrogenism, and inflammation, single-agent therapy is less successful 101. Synergistic interactions may improve therapeutic results, according to studies on herbal mixtures. For instance, as compared to individual herbs, formulations including Trigonella foenum-graecum and Cinnamomum verum have shown enhanced insulin sensitivity and glycemic management. Combinations of Tinospora cordifolia and Withania somnifera also exhibit increased anti-inflammatory and antioxidant properties, which may improve ovarian function 102. Such combinations are more beneficial than monotherapy in improving lipid profiles, hormonal balance, and menstrual regularity, according to limited clinical and experimental research. Nevertheless, there are presently few reliable large-scale clinical trials, and more investigation is required to confirm these synergistic benefits and provide standardized formulations 103.
Commercial Herbal Formulations: Because of their multi-targeted effects on hormonal imbalance and metabolic dysfunction, commercial herbal preparations are becoming more and more popular as supplemental treatments for Polycystic Ovary Syndrome. These formulations, which frequently include many medicinal plants with established endocrine and metabolic advantages, are offered in a variety of dosage forms, including capsules, tablets, syrups, and powders. Herbs including Withania somnifera, Asparagus racemosus, Trigonella foenum-graecum, and Cinnamomum species are used in Ayurvedic and nutraceutical products to increase insulin sensitivity, control menstrual cycles, and lower androgen levels. To improve therapeutic results, some commercial formulations may include substances like curcumin, berberine, or inositol in addition to plant extracts 104. Such formulations may assist improve ovulatory function, restore hormonal balance, and regulate metabolic markers, according to preclinical and limited clinical research. However, the main obstacles continue to be composition heterogeneity, a lack of standardization, and a dearth of large-scale clinical trials. Consequently, even though commercial herbal treatments have potential, their usage should be supervised by medical professionals to guarantee efficacy and safety 105.
Clinical Evidence and Research Studies: Although it is still small in scope, clinical data regarding the use of herbal and alternative medicines to treat Polycystic Ovary Syndrome has increased recently. Numerous pilot and randomized studies indicate that plant-based therapies have positive impacts on hormonal and metabolic markers. For example, in women with PCOS, supplementing with Cinnamomum verum has been linked to enhanced menstrual cyclist and insulin sensitivity. Similarly, Camellia sinensis has been shown to have beneficial effects on oxidative stress reduction and weight management 106. Ovarian morphology and menstrual cycle regularity have improved in clinical trials using extracts from the seeds of Trigonella foenum-graecum. Additionally, some research reports improved ovulatory function and decreased androgen levels when combined herbal or nutraceutical therapy are used. However, the majority of research have inconsistent methodology, small sample sizes, and brief durations 107. Therefore, even though preliminary results are encouraging, more thorough, extensive clinical trials are needed to prove long-term efficacy, safety, and standardization 108.
In-vitro and In-vivo Studies: Understanding the etiology and management of polycystic ovarian syndrome (PCOS) depends heavily on both in-vitro and in-vivo research. Cultured ovarian theca and granulosa cells are commonly used in in-vitro investigations to study mechanisms including insulin resistance, altered steroidogenesis, and androgen overproduction. Increased luteinizing hormone (LH) stimulation and insulin signaling boost androgen production, which contributes to follicular arrest, according to these researches. Furthermore, in-vitro tests aid in assessing how pharmaceuticals like metformin and anti-androgens affect cellular reactions 109. In-vivo research on humans and animal models offers a more thorough comprehension of PCOS as a systemic illness. Key characteristics of PCOS, such as anovulation, cystic ovaries, and metabolic abnormalities, are mimicked in rodent models produced with androgens or high-fat diets. These models are useful for evaluating long-term results and therapeutic approaches. The involvement of hyperinsulinemia, chronic inflammation, and genetic susceptibility in the development of PCOS have been emphasized by clinical in-vivo research in women with the condition 110. When combined, in-vitro and in-vivo methods enhance the clinical management of PCOS and allow for the creation of targeted treatments 111.
Clinical Trials and Human Studies: The advancement of Polycystic Ovary Syndrome diagnosis and treatment depends on human studies and clinical trials. The safety and effectiveness of pharmaceutical, lifestyle, and novel therapy approaches in afflicted women are assessed in these researches. Insulin-sensitizing medications like metformin have been shown in randomized controlled trials (RCTs) to increase ovulatory function, lower androgen levels, and improve metabolic outcomes. Clinical research on combined oral contraceptives also supports its ability to control menstrual periods and lessen hyperandrogenic symptoms such acne and hirsutism 112. Trials using lifestyle interventions, such as diet and exercise, typically demonstrate improvements in body weight, insulin sensitivity, and reproductive function, underscoring their importance as first-line treatment. Novel therapies including inositols and glucagon-like peptide-1 (GLP-1) receptor agonists, which show encouraging effects on metabolic and hormonal parameters, have been investigated in more recent human research. The long-term hazards of PCOS, such as type 2 diabetes, cardiovascular disease, and infertility, are further revealed by large cohort and observational studies 113. All things considered, human research and clinical trials make a substantial contribution to evidence-based recommendations, allowing for individualized and successful PCOS treatment plans for women 114.
Comparative Effectiveness with Conventional Drugs: In Polycystic Ovary Syndrome, comparative effectiveness studies assess how innovative or alternative treatments compare to traditional medications in terms of improving metabolic and reproductive outcomes. Metformin for insulin resistance and combination oral contraceptives (COCs) for hyperandrogenism and menstrual control are examples of standard pharmacological therapies. Metformin and lifestyle modifications both increase insulin sensitivity and ovulation rates, but combination strategies frequently produce better outcomes, according to clinical investigations 115. Insulin-sensitizing drugs may be more effective at treating metabolic problems than COCs, but they are less successful at quickly controlling symptoms like hirsutism and acne. Recent research has contrasted metformin with novel treatments such as inositols and GLP-1 receptor agonists. While GLP-1 receptor agonists offer higher weight loss and metabolic advantages in obese women with PCOS, myo-inositol has demonstrated comparable efficacy in restoring ovulation with less gastrointestinal side effects 116. When used with COCs, anti-androgens like spirolactone have been shown to reduce hirsutism more effectively. All things considered, comparative effectiveness research shows that there is no one medication that is always better; rather, treatment should be customized according to the patient's symptoms, metabolic risk, and reproductive objectives. A customized, multimodal strategy to PCOS care is supported by these data 117.
Pharmacokinetics and Bioavailability of Herbal Compounds: A complex endocrine condition linked to insulin resistance, hyperandrogenism, and persistent inflammation is called polycystic ovarian syndrome (PCOS). Because of their antioxidant, anti-inflammatory, and insulin-sensitizing properties, herbal substances such berberine, resveratrol, quercetin, and apigenin have demonstrated therapeutic potential. However, pharmacokinetics and bioavailability have a significant impact on their therapeutic efficacy 118. Absorption, distribution, metabolism, and excretion are all components of pharmacokinetics (ADME). Due to their low solubility in water and restricted intestinal permeability, the majority of phytochemicals show poor absorption. Furthermore, these substances may be metabolized by gut microbes prior to systemic absorption, which would further lower bioavailability. After being absorbed, these substances spread to reproductive and metabolic tissues such the ovaries, liver, and adipose tissue, where they have therapeutic effects 119. One important factor limiting efficacy is metabolism.
Cytochrome P450 enzymes in the liver undertake substantial first-pass metabolism of herbal substances, resulting in metabolites that may be less active or quickly removed. As a result, systemic concentrations stay low, which lessens the pharmacological effect. Renal and biliary pathways are the main routes of excretion. One of the primary obstacles to PCOS phytotherapy is still poor oral bioavailability. Variability in herbal formulations, fast metabolism, and chemical instability are some of the factors that lead to inconsistent medicinal results. For instance, flavonoids with strong biological activity, such as apigenin and ellagic acid, have limited therapeutic efficacy because of their poor systemic availability 120. Strategies including phytosomes, lipid-based delivery systems, and nanoformulations have been developed to improve solubility and absorption in order to get around these restrictions. These methods enhance therapeutic efficacy and pharmacokinetic characteristics. In conclusion, enhancing the pharmacokinetic characteristics and bioavailability of herbal substances is crucial for their successful clinical application, even though they present promising multi-target therapeutic alternatives for PCOS 121.
Safety, Toxicity, and Herb–Drug Interactions: Pharmaceuticals including insulin sensitizers, oral contraceptives, and antiandrogens are frequently used to treat polycystic ovarian syndrome (PCOS), but many patients also use herbal therapies, which raises questions regarding safety and toxicity. For hormonal balance and glycemic control, botanicals like ashwagandha, fenugreek, licorice, and cinnamon are commonly utilized. Their safety profiles vary, nevertheless. For instance, licorice can produce pseudoaldosteronism, which can result in hypertension, hypokalemia, and fluid retention, whereas cassia cinnamon contains coumarin, which can be harmful to the liver when ingested in excess. Fenugreek may cause gastrointestinal distress and hypoglycemia in those who are vulnerable, while ashwagandha is generally regarded as harmless but has been connected to few incidences of liver damage 122. One major clinical problem in the treatment of PCOS is herb-drug interactions. Numerous herbal substances can affect drug transport systems and cytochrome P450 enzymes, changing the pharmacokinetics of prescription drugs. For example, fenugreek and cinnamon may intensify metformin's glucose-lowering effects, raising the risk of hypoglycemia. Licorice may worsen potassium loss and raise blood pressure by intensifying the effects of corticosteroids and diuretics. Additionally, when used in conjunction with hormone therapy, herbs with antiandrogenic qualities like spearmint may have additive benefits, but there is currently little solid clinical evidence for such interactions 123. Healthcare professionals must evaluate the usage of herbal supplements in PCOS patients and offer evidence-based recommendations in light of these hazards. Patients should be urged to follow prescribed dosage guidelines, use standardized goods, and report any side effects right away. To reduce dangers, better pharmacovigilance and increased knowledge of herb-drug interactions are required. Although certain herbal remedies appear promising, their incorporation into the treatment of PCOS should be done carefully, with a personalized risk-benefit analysis and close observation 124.
Regulatory Aspects and Standardization of Herbal Medicines: Due to variations in content, quality, and efficacy data, regulatory control and standardization of herbal remedies used to treat polycystic ovarian syndrome (PCOS) continue to be difficult. Many herbal products are sold as dietary supplements and do not go through the same stringent pre-market approval procedures as traditional pharmaceuticals. The Dietary Supplement Health and Education Act (DSHEA), which lays the burden of safety and labeling on producers rather than requiring proof of efficacy prior to marketing, is how the U.S. Food and Drug Administration governs herbal supplements in places like the United States. The European Medicines Agency, on the other hand, offers a framework for traditional herbal medicinal products that emphasizes quality, safety, and traditional use, albeit with fewer strict clinical requirements than those for contemporary pharmaceuticals 125. For herbal formulations used to treat PCOS to be consistent from batch to batch, standardization is essential. The concentration of active ingredients can be considerably changed by variations in plant species, growth circumstances, harvesting techniques, and extraction techniques. To enhance the quality and safety of herbal medicines, organizations like the World Health Organization have created recommendations for good manufacturing practices (GMP) and good agriculture and collection practices (GACP). Identifying bioactive markers, managing contaminants (such as heavy metals and pesticides), and making sure that dosage and ingredient labels are correct are all common components of standardization. Nonetheless, there are still a lot of products on the market that lack sufficient quality control and standardization 126. Clinical results and patient safety are directly impacted by these regulatory and standards challenges in the setting of PCOS. Integrating herbal remedies into evidence-based care is made more difficult by the lack of worldwide standards. To guarantee the safety, efficacy, and consistent quality of herbal medications used for PCOS, regulatory frameworks must be strengthened, clinical trials must be encouraged, and pharmacovigilance systems must be improved 127.
Challenges and Limitations in Herbal Therapy for PCOS: Although herbal therapy is frequently used as an adjunctive treatment for polycystic ovarian syndrome (PCOS), it has a number of significant drawbacks. The dearth of high-quality clinical evidence is one of the main problems. There are few large-scale randomized controlled trials, despite the fact that numerous herbs, including ashwagandha, spearmint, and cinnamon, have demonstrated possible benefits in tiny or exploratory investigations. Establishing certain efficacy, ideal dosage, and long-term safety is challenging as a result. Furthermore, it is difficult to generalize the results of herbal treatments due to the heterogeneity of PCOS itself, which varies in symptoms including insulin resistance, hyperandrogenism, and ovulatory dysfunction 128. The problem of standardization and quality control is another significant constraint. Depending on plant species, growth circumstances, harvesting techniques, and extraction procedures, the composition of herbal products might vary greatly. Many commercially marketed medicines lack constant amounts of active substances, despite recommendations from organizations such as the World Health Organization. Safety issues are further raised by contamination with pesticides, adulterants, or heavy metals. Additionally, insufficient or deceptive labeling makes it challenging for patients and physicians to evaluate the dependability and quality of the product 129. Integrating herbal medicine into PCOS management is complicated by herb-drug interactions and safety issues. Many patients take traditional drugs like metformin or hormonal contraceptives in addition to herbal therapies, which raises the possibility of interactions that could change the effectiveness of the prescription or have negative side effects. There is variation in the safety and efficacy of herbal supplements due to regulatory restrictions, especially under frameworks like those of the U.S. Food and Drug Administration, which do not require thorough pre-market assessment. Stronger regulatory control, better clinical research, and increased patient and healthcare provider knowledge are all necessary to address these issues 130. However, because they can improve insulin sensitivity, reduce oxidative stress, and restore endocrine system control, bioactive phytochemicals such as flavonoids, polyphenols, alkaloids, terpenoids, and saponins have given hope in the field of disease treatment. The stability, bioavailability, and targeted administration of phytochemicals are being positively impacted by recent advancements in nanocarrier systems, such as polymeric nanoparticles and antibody-conjugated formulations 131.
Future Perspectives and Research Directions: Future studies on polycystic ovarian syndrome (PCOS) will increasingly concentrate on enhancing long-term illness management, individualized treatment, and early identification. It is anticipated that developments in proteomics, metabolomics, and genomes will improve knowledge of PCOS pathophysiology, especially the intricate interactions between insulin resistance, hyperandrogenism, and chronic inflammation. These methods, which go beyond the conventional standards set by the Rotterdam consensus group, may aid in the discovery of new biomarkers for early detection and allow for a more accurate classification of PCOS phenotypes. In the end, this might enable customized treatment plans based on each patient's unique metabolic and hormonal characteristics 132. The creation of multidisciplinary and integrative therapeutic methods is another promising avenue. The use of lifestyle modifications, nutraceuticals, and evidence-based herbal medicine in conjunction with traditional therapy like insulin sensitizers and hormone treatments is becoming more popular.
In order to assess the effectiveness, safety, and mechanisms of herbal therapy in PCOS, future research should give priority to carefully planned randomized controlled trials. Additionally, mobile applications and digital health tools may enhance long-term monitoring, symptom tracking, and patient adherence, providing better patient-centered care 133. Lastly, improving PCOS management requires filling in gaps in international healthcare access and legal frameworks. To guarantee safety and effectiveness, improved pharmacovigilance systems, harmonized international norms, and standardization of herbal products are required. Research and policy development in this field are greatly aided by organizations like the World Health Organization. In order to provide comprehensive care, future studies should also take into account the psychosocial effects of PCOS, such as mental health and quality of life. In general, the future of PCOS management will be shaped by a confluence of clinical research, scientific innovation, and legislative reform 134.
CONCLUSION: The current definition, epidemiology, pathophysiology, clinical therapy, and long-term health hazards of PCOS were all covered in this article. The etiology of PCOS is not entirely explained by insulin resistance, despite the theory that it is the primary metabolic abnormality. This is by no means an exhaustive review. There will only be a fresh consensus meeting and a thorough report with stringent recommendations. It is commonly known that H-PCOS and the metabolic syndrome are closely related, however it appears that HH-PCOS is not. On the other hand, in about 85% of instances, the HH-phenotype shows signs of an overactive immune system, this is primarily defined by inflammation and autoimmunity. PCOS has been uniformly linked to chronic low-grade inflammation, but one must question whether this generalization is not, once again, solely based on patient selection biases from mixed studies of phenotype A and phenotype D PCOS patients. The fact that immune system hyperactivity in HH-PCOS considerably surpasses what has been shown for PCOS in general lends credence to this interpretation. Menstrual cycle regulation, ovulation induction, insulin resistance, hyperandrogenism, and obesity-related PCOS are all treated with medications. Many medications are used to treat PCOS with a variety of symptoms, however effective PCOS therapy is still difficult. Numerous potential therapeutic benefits for polycystic ovarian syndrome, insulin resistance, hyperandrogenism, oligo/amenorrhea, and obesity have been assessed for some medicinal herbs. Therefore, more pre-clinical and clinical studies are required to examine the effectiveness of herbal drugs in PCOS. The effectiveness of medicinal plants in the management and treatment of polycystic ovarian syndrome is better understood thanks to this review.
Significant and long-lasting weight loss and improvements in obesity-related comorbidities are the outcomes of bariatric surgery. Randomized controlled trials are required, but non-randomized research indicate that bariatric surgery may be crucial in the treatment of patients with PCOS and/or endometrial hyperplasia. The discipline of bariatric surgery is growing and providing long-term outcomes for both weight loss and co-morbidity remission. The effectiveness of nutritional supplements and herbal medicines for PCOS symptoms is not supported by high-quality research, and there is insufficient proof of their safety. Inositol and omega-3 fish oil supplements, however, may be beneficial for women with PCOS, according to some low-quality research. More investigation is required. There is increasing agreement that aberrant gonadotrophin dynamics, androgen excess, and insulin resistance are the main characteristics. Sometimes a familial pattern indicates a genetic component, but the potential genes are yet unknown. PCOS has been linked to endometrial cancer, diabetes mellitus, obesity, and cardiovascular disease, with both immediate and long-term effects. Even though PCOS has significant negative health effects, most women are sadly unaware of these concerns. The clinician's primary goal should be to identify and treat the metabolic consequences of PCOS as soon as possible. A balanced diet and regular exercise are the two most important lifestyle changes. In this regard, PCOS is a prime example of a pathology where its usual long-term consequences can be avoided or postponed with early identification and treatment. Treating hirsutism and restoring ovulation have historically been the main goals of PCOS therapy. However, as insulin resistance and hyperinsulinemia are frequently linked to the pathophysiology of the syndrome, it should be given more consideration. Researchers should consider more suitable methods for managing the metabolic changes associated with PCOS because these changes have significant long-term effects on health. The main therapy recommendation for PCOS-related infertility should be lifestyle modifications before considering any medication choices. Current research indicates that while PCOS has no effect on the risk of breast or ovarian cancer, it raises the risk of endometrial cancer in women of all ages. These results suggest that PCOS may contribute to the morbidity of gynecological cancer. Although vitamin D and inositol may be good for one's health, further research and guidance are needed. The effectiveness of alternative therapies has not been conclusively demonstrated. While PCOS metabolic dysfunction has long been treated with insulin sensitizers like metformin, more recent medications like incretin mimetics and SGLT2 inhibitors have shown greater efficacy in lowering weight and cardiovascular risk.
Another possibility is that the body rests in a chronic inflammatory state due to the breakdown of immunological tolerance, which impacts follicular ovulation, development, and generation. Exercise, an oral insulin sensitizer, anti-inflammatory drugs like metformin, and oral contraceptives has been the main treatments for PCOS clinical symptoms in recent years. These treatments have all improved the short-term prognosis of ovulation. Casually, as early environmental intervention is more likely to assist women with high genetic loading. When a patient states that both her mother and sister have the illness, this is more than just a box to check on an intake form; it's a hint that active lifestyle counseling should start right away, ideally before the complete phenotypic manifests.
ACKNOWLEDGEMENT: Nil
CONFLICT OF INTEREST: Nil
REFERENCES:
- Management D: Pcod of Pharmaceutical neutraceutical: enriched low- glycemic muffins for. World J Pharm Res 2025; 14(23): 918–36.
- El Hayek S, Bitar L, Hamdar LH, Mirza FG and Daoud G: Poly Cystic Ovarian Syndrome: An updated overview. Front Physiol 2016; 7(4): 1–15.
- Deepak Kumar K, Huntriss R, Green E, Bora S and Pettitt C: Development of a nutrition screening tool to identify need for dietetic intervention in female infertility. J Hum Nutr Diet 2023; 36(1): 154–68.
- Della Corte L, Foreste V, Barra F, Gustavino C, Alessandri F and Centurioni MG: Current and experimental drug therapy for the treatment of polycystic ovarian syndrome. Expert Opin Investig Drugs [Internet]. 2020; 29(8): 819–30. Available from: https://doi.org/10.1080/13543784.2020.1781815
- Coutinho EA and Kauffman AS: The Role of the Brain in the Pathogenesis and Physiology of Polycystic Ovary Syndrome (PCOS). Med Sci (Basel, Switzerland) 2019; 7(8).
- Hiam D, Moreno-Asso A, Teede HJ, Laven JSE, Stepto NK and Moran LJ: The genetics of polycystic ovary syndrome: An overview of candidate gene systematic reviews and genome-wide association studies. J Clin Med 2019; 8(10).
- Hu C, Pang B, Ma Z and Yi H: Immunophenotypic profiles in polycystic ovary syndrome. Mediators Inflamm 2020; 2020.
- He FF and Li YM: Role of gut microbiota in the development of insulin resistance and the mechanism underlying polycystic ovary syndrome: A review. J Ovarian Res 2020; 13(1): 1–13.
- Kumari R, Singh RK and Garg A: “Herbal plants used in the treatment of PCOS-A Comprehensive review.” Int J Pharma Prof Res 2024; 15(1): 57–71.
- Zehravi M, Maqbool M and Ara I: Healthy Lifestyle and Dietary Approaches to Treating Polycystic Ovary Syndrome: A Review. Open Heal 2022; 3(1): 60–5.
- Ghazeeri GS, Nassar AH, Younes Z and Awwad JT: Pregnancy outcomes and the effect of metformin treatment in women with polycystic ovary syndrome: An overview. Acta Obstet Gynecol Scand 2012; 91(6): 658–78.
- Collée J, Mawet M, Tebache L, Nisolle M and Brichant G: Polycystic ovarian syndrome and infertility: overview and insights of the putative treatments. Gynecol Endocrinol [Internet] 2021; 37(10): 869–74. Available from: https://doi.org/10.1080/09513590.2021.1958310
- Ganie MA, Sahar T, Rashid A, Wani IA, Nisar S and Sathyapalan T: Comparative Evaluation of Biomarkers of Inflammation Among Indian Women With Polycystic Ovary Syndrome (PCOS) Consuming Vegetarian vs. Non-vegetarian Diet. Front Endocrinol (Lausanne) 2019; 10(11): 1–11.
- Azziz R: Introduction: Determinants of polycystic ovary syndrome. Fertil Steril 2016; 106(1): 4–5.
- Bergh CM, Moore M and Gundell C: Evidence-Based Management of Infertility in Women with Polycystic Ovary Syndrome. JOGNN 2016; 45(1): 111–22.
- Ahmed S, Rahman MS, Jahan I, Kaiser MS, Hosen ASMS and Ghimire D: A Review on the Detection Techniques of Polycystic Ovary Syndrome Using Machine Learning. IEEE Access 2023; 11(8): 86522–43.
- Ashraf S, Nabi M, Rasool Sul A, Rashid F and Amin S: Hyperandrogenism in polycystic ovarian syndrome and role of CYP gene variants: a review. Egypt J Med Hum Genet 2019; 20(1).
- Ajmal N, Khan SZ and Shaikh R: Polycystic ovary syndrome (PCOS) and genetic predisposition: A review article. Eur J Obstet Gynecol Reprod Biol X [Internet] 2019; 3: 100060. Available from: https://doi.org/10.1016/j.eurox.2019.100060
- Abdalla MA, Deshmukh H, Atkin S and Sathyapalan T: A review of therapeutic options for managing the metabolic aspects of polycystic ovary syndrome. Ther Adv Endocrinol Metab 2020; 11: 1–19.
- Abdalla M, Deshmukh H, Atkin SL and Sathyapalan T: miRNAs as a novel clinical biomarker and therapeutic targets in polycystic ovary syndrome (PCOS): A review. Life Sci [Internet] 2020; 259(7): 118174. Available from: https://doi.org/10.1016/j.lfs.2020.118174
- Aboeldalyl S, James C, Seyam E, Ibrahim EM, Shawki HED and Amer S: The role of chronic inflammation in polycystic ovarian syndrome a systematic review and meta-analysis. Int J Mol Sci 2021; 22(5): 1–31.
- Clark AK, Haas KN and Sivamani RK: Edible plants and their influence on the gut microbiome and acne. Int J Mol Sci 2017; 18(5).
- Raut SH and Gadani MC: Comparative characterization study of plant based calcium versus synthetic calcium. Int J Pharm Chem Anal 2021; 8(3): 134–40.
- Calcaterra V, Verduci E, Cena H, Magenes VC, Todisco CF and Tenuta E: Polycystic ovary syndrome in insulin‐resistant adolescents with obesity: The role of nutrition therapy and food supplements as a strategy to protect fertility. Nutrients 2021; 13(6): 1–32.
- Cassar S, Misso ML, Hopkins WG, Shaw CS, Teede HJ and Stepto NK: Insulin resistance in polycystic ovary syndrome: A systematic review and meta-analysis of euglycaemic-hyperinsulinaemic clamp studies. Hum Reprod 2016; 31(11): 2619–31.
- Waghmare S V and Shanoo A: Polycystic Ovary Syndrome: A Literature Review with a Focus on Diagnosis, Pathophysiology, and Management. Polycystic Ovary Syndr 2023; 15(10): 1–9.
- Shayan A, Shobeiri F, Khalili A and Masoumi SZ: The Effect of Agnugol Tablet on Oligomenorrhea in Patients with Polycystic Ovary Syndrome: A Clinical Trial. Heal Spiritual Med Ethics 2017; 4(1): 22–7.
- Tsilchorozidou T, Overton C and Conway GS: The pathophysiology of polycystic ovary syndrome. Clin Endocrinol (Oxf) 2004; 60(1): 1–17.
- Jones MR and Goodarzi MO: Genetic determinants of polycystic ovary syndrome: progress and future directions. Fertil Steril [Internet] 2016; 106(1): 25–32. Available from: http://dx.doi.org/10.1016/j.fertnstert.2016.04.040
- Azziz R: Polycystic Ovary Syndrome. Obstet Gynecol [Internet] 2018; 132(2). Available from: https://journals.lww.com/greenjournal/fulltext/2018/08000/polycystic_ovary_syndrome.9.aspx
- Rosenfield RL and Ehrmann DA: The Pathogenesis of Polycystic Ovary Syndrome (PCOS): The hypothesis of PCOS as functional ovarian hyperandrogenism revisited. Endocr Rev 2016; 37(5): 467–520.
- Teede HJ, Misso ML, Costello MF, Dokras A, Laven J and Moran L: Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum Reprod 2018; 33(9): 1602–18.
- Diamanti-Kandarakis E and Dunaif A: Insulin resistance and the polycystic ovary syndrome revisited: An update on mechanisms and implications. Endocr Rev 2012; 33(6): 981–1030.
- Khuri RN, Agulian SK and Bogharian KK: Intracellular bicarbonate of skeletal muscle under different metabolic states. Am J Physiol 1976; 230(1): 228–32.
- González F: Inflammation in Polycystic Ovary Syndrome: Underpinning of insulin resistance and ovarian dysfunction. Steroids 2012; 77(4): 300–5.
- Duleba AJ and Dokras A: Is PCOS an inflammatory process? Fertil Steril 2012; 97(1): 7–12.
- De Leo V, Musacchio MC, Cappelli V, Massaro MG, Morgante G and Petraglia F: Genetic, hormonal and metabolic aspects of PCOS: An update. Reprod Biol Endocrinol [Internet] 2016; 14(1): 1–17. Available from: http://dx.doi.org/10.1186/s12958-016-0173-x
- Meier L and Brunner S: Genetic and environmental factors contributing to polycystic ovary syndrome (PCOS): An endocrine perspective. Intern ional J Endocrinol Res 2026; 8(1): 18–25.
- Diamanti-Kandarakis E, Piperi C, Spina J, Argyrakopoulou G, Papanastasiou L and Bergiele A: Polycystic ovary syndrome: the influence of environmental and genetic factors. Hormones (Athens) 2006; 5(1): 17–34.
- Arentz S, Smith CA, Abbott J and Bensoussan A: Nutritional supplements and herbal medicines for women with polycystic ovary syndrome ; a systematic review and meta-analysis. Arentz al BMC CAM 2017; 1–14.
- Patel S. Journal of Steroid Biochemistry and Molecular Biology Polycystic ovary syndrome (PCOS), an in fl ammatory, systemic, lifestyle endocrinopathy. J Steroid Biochem Mol Biol [Internet] 2018; (2): 0–1. Available from: http://dx.doi.org/10.1016/j.jsbmb.2018.04.008
- Grant P: Spearmint Herbal Tea has Signifi cant Anti-androgen Effects in Polycystic Ovarian Syndrome. A Randomized Controlled Trial. Spearmint Herb Tea has Signifi cant Anti-androgen Eff Polycystic Ovarian Syndr 2010; 188(2009): 186–8.
- Info A: Suggested herbal remedies effective on polycystic ovarian syndrome from the viewpoint of Persian medicine. J Med Plants J 2022; 21(9): 1–10.
- Azziz R, Carmina E, Dewailly D, Escobar-morreale F and Ph D: The Androgen Excess and PCOS Society criteria for the polycystic ovary syndrome: the complete task force report 2009; 91.
- Arun PP, Kumar G, Tiwari RK and Sharma B: Herbal-based medicine approach in the treatment of infertility: a review. Lejana J 2025; 8(11): 103–28.
- Ali BH, Blunden G, Tanira MO and Nemmar A: Some phytochemical, pharmacological and toxicological properties of ginger (Zingiber officinale Roscoe): A review of recent research. Food Chem Toxicol 2008; 46: 409–20.
- Teede HJ, Misso ML, Boyle JA, Garad RM, Mcallister V and Downes L: Translation and implementation of the Australian-led PCOS guideline: clinical summary and translation resources from the International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome. Transl Implement Aust PCOS Guidel 3–24.
- Ye Y, Liu X, Wu N, Han Y, Wang J and Yu Y: Efficacy and Safety of Berberine Alone for Several Metabolic Disorders: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Efficacy Saf Berberine Alone Sev Metab Disord 2021; 12(4): 1–9.
- Rani R, Chitme HR, Kukreti N, Pant P and Abdel-wahab BA: Regulation of Insulin Resistance, Lipid Profile and Glucose Metabolism Associated with Polycystic Ovary Syndrome by. Tinospora cordifolia Nutr 2023;
- Arentz S, Abbott JA, Smith CA and Bensoussan A: Herbal medicine for the management of polycystic ovary syndrome (PCOS) and associated oligo/ amenorrhoea and hyperandrogenism; a review of the laboratory evidence for effects with corroborative clinical findings. BMC Complement Altern Med [Internet] 2014; 14(511): 1–19. Available from: http://www.biomedcentral.com/1472-6882/14/511
- Bykowska-Derda A, Kaluzna M, Ruchała M, Ziemnicka K and Czlapka-Matyasik M: The Significance of Plant-Based Foods and Intense Physical Activity on the Metabolic Health of Women with PCOS: A Priori Dietary-Lifestyle Patterns Approach. Appl Sci 2023; 13(4).
- Ndarakis E, Argyrakopoulou G, Economou F, Kandaraki E and Koutsilieris M: Diamanti-ka Journal of Steroid Biochemistry and Molecular Biology Defects in insulin signaling pathways in ovarian steroidogenesis and other tissues in polycystic ovary syndrome (PCOS) Defects in insulin signaling pathways in ovarian steroidogenesis and other tissues in polycystic ovary syndrome (PCOS). J Steroid Biochem Mol Biol 2008; 109: 242–6.
- Kwon CS, Seoane-vazquez E and Rodriguez-monguio R: FDA safety actions for antidiabetic drugs marketed in the US, 1980 – 2015. Int J Risk Saf Med 2017; 28(2016): 197–211.
- Aranha I: Polycystic Ovarian Syndrome (PCOS), A Distress of Female Reproductive Health. Int J Arts, Sci Humanit Polycystic 2019; 8(1): 46–53.
- Escobar F: Polycystic ovary syndrome: definition, aetiology, diagnosis and treatment. Héctor F Escobar-Morreale 2018; 14(5).
- Azziz R: Corrigendum PCOS in 2015 : New insights into the genetics of polycystic ovary syndrome. Nat Publ Gr [Internet] 2016; 75: 2016. Available from: http://dx.doi.org/10.1038/nrendo.2016.9
- Daryani S: The role of fiber supplementation in the management and a Thesis Presented to the Faculty of the Weill Cornell Graduate School of Medical 2020.
- Ainehchi N, Farshbaf-khalili A, Ghasemzadeh A, Hamdi K and Khaki A: The effect of herbal medicine supplementation on clinical and para-clinical outcomes in women with PCOS: a systematic review and meta-analysis. Int J Women’s Heal Reprod Sci 2019; 7(5): 423–33.
- Gateva A, Unfer V and Kamenov Z: The use of inositol (s) isomers in the management of polycystic ovary syndrome : a comprehensive review. Gynecol Endocrinol [Internet] 2018; 0(0): 1–6. Available from: https://doi.org/10.1080/09513590.2017.1421632
- Ilaria S, Tommaso O, Chiara A, Roberto M and Donatella C: Acceptcrt Curr Med Res Opin [Internet] 2020; 0(0): 000. Available from: http://dx.doi.org/10.1080/03007995.2020.1729108
- Mykhalchenko K, Lizneva D, Trofimova T, Walker W, Suturina L and Diamond MP: Genetics of polycystic ovary syndrome. Expert Rev Mol Diagn [Internet] 2017; 0(0). Available from: http://dx.doi.org/10.1080/14737159.2017.1340833
- Azziz R: Síndrome de ovario poliquístico. Obstet Gynecol 2018; 1: 1–21.
- Latha KRS: A comprehensive method for management PCOD and PCOS: comparison of conventional and contemporary healthcare systems. BTS Int Adv Pharm Sci J 2026; 01(03): 1–32.
- Considine R V, Abdelhadi OA and Acton AJ: Inflammation triggered by saturated fat ingestion is linked to insulin resistance and hyperandrogenism in PCOS. J Clin Endocrinol Metab 2020;
- Wawrzkiewicz-Jałowiecka A, Kowalczyk K, Trybek P, Jarosz T, Radosz P and Setlak M: In search of new therapeutics—molecular aspects of the pcos pathophysiology: Genetics, hormones, metabolism and beyond. Int J Mol Sci 2020; 21(19): 1–24.
- Kathleen M Hoeger, Anuja Dokras and Terhi Piltonen: P. Update on PCOS: Consequences, Challenges and Guiding Treatment. Updat PCOS Consequences, Challenges Guid Treat 2020.
- Araújo BS, Baracat MCP, Simões S, Nuñes CDO, Arantes G and Maciel R: Kisspeptin influence on polycystic ovary syndrome - a mini review. Reprod Sci 2020;
- Parker J: Pathophysiological Effects of Contemporary Lifestyle on Evolutionary-Conserved Survival Mechanisms that Disturb the Hallmarks of Health in Polycystic Ovary Syndrome 2023; (3).
- Miller WL: Pathophysiology, genetics, and treatment of hyperandrogenism. Pediatr Clin North Am 1997; 44(2): 375–95.
- Lopresti AL, Smith SJ, Malvi H and Kodgule R: An investigation into the stress-relieving and pharmacological actions of an ashwagandha (Withania somnifera) extract. Lopresti al Med 2019; 37(8).
- Article R: PCOS Review and literature. Rev Assoc Med BRAs [Internet] 2016; 62(9): 867–71. Available from: https://www.scielo.br/pdf/ramb/v62n9/0104-4230-ramb-62-9-0867.pdf
- Charalampakis V, Tahrani AA, Helmy A, Gupta JK and Singhal R: Polycystic ovary syndrome and endometrial hyperplasia: an overview of the role of bariatric surgery in female fertility. Eur J Obstet Gynecol Reprod Biol [Internet] 2016; 207: 220–6. Available from: http://dx.doi.org/10.1016/j.ejogrb.2016.10.001
- Effect H, Fenugreek OF, In S and Subjects DD: Copyright (c) 1990 Pergamon Press plc. All rights reserved. Nutr Res 1990; 10(c): 731–9.
- Taylor P and Srinivasan K: Fenugreek (Trigonella foenum- graecum): A Review of Health Beneficial Physiological Effects Fenugreek (Trigonella foenum-graecum): A Review. Food Rev Int 2007; (2013): 37–41.
- Venkata KCN, Swaroop A, Bagchi D and Bishayee A: R EVIEW A small plant with big benefits : Fenugreek (Trigonella foenum-graecum Linn.) for disease prevention and. Mol Nutr Food Res 2017; 61: 1600950: 1–26.
- Ulbricht C, Basch E, Burke D, Cheung L, Ernst E and Kuo G: Fenugreek (Trigonella foenum-graecum L . Leguminosae): An Evidence-Based Systematic Review by the Natural Standard Research Collaboration 20077; 7: 143–177.
- Armanini D, Jung M, Fiore C, Bonanni G, Scaroni C and Sartorato P: Licorice reduces serum testosterone in healthy women. D Arman al / Steroids 2004; 69: 763–6.
- Wang ZY, Nixon DW, Wang ZY and Nixon DW: Licorice and Cancer Licorice and Cancer. Nutr Cancer 2016; 5581(12).
- Ashkar F, Rezaei S, Salahshoornezhad S, Vahid F and Gholamalizadeh M: The Role of medicinal herbs in treatment of insulin resistance in patients with Polycystic Ovary Syndrome : A literature review. Fatemeh Ashkar a. 2020; 57–75.
- Nutrition H and Cycle L: Wisconsin Nutrition Certification Course 2025;
- Utility P, Family A and Physicians M: Family Doctor. A J New York State Acad Fam Physicians 2025;
- Al MAET, Akdo M, Tamer MN, Cüre E, Cüre MC and Köro K: Effect of Spearmint (Mentha spicata Labiatae) Teas on Androgen Levels in Women with Hirsutism Phyther Res 2007; 447(2): 444–7.
- Machrafi S El, Elkouali M, Sadia T, Iskandar S, Rahhal R and Bouhadi M: Phytochemical composition and antioxidant activities of Mentha spicata L. and Melissa officinalis L. from the Settat region of Morocco: A comparative study of extraction methods. J Ecol Eng 2025; 26(12): 164–77.
- Mckay DL and Blumberg JB: Review article a review of the bioactivity and potential health benefits of chamomile tea (Matricaria recutita L .). Phyther Res 2006; 530: 519–30.
- Kumar V, Sachan R, Rahman M, Sharma K and Anwar F: Prunus amygdalus extract exert antidiabetic effect via inhibition of DPP-IV: in-silico and in-vivo approaches. J Biomol Struct Dyn [Internet] 2020; 0(0): 1–15. Available from: https://doi.org/10.1080/07391102.2020.1775124
- Effect of Aloe barbadensis Mill. formulation on Letrozole induced polycystic ovarian syndrome rat model. J Ayurveda Integr Med 2010; 1(4): 273–9.
- Patel DK, Kumar R, Laloo D and Hemalatha S: Natural medicines from plant source used for therapy of diabetes mellitus : An overview of its pharmacological aspects. Asian Pacific J Trop Dis [Internet] 2012; 2(3): 239–50. Available from: http://dx.doi.org/10.1016/S2222-1808(12)60054-1
- Nagao T, Hase T and Tokimitsu I: Diet and Physical Activity A Green Tea Extract High in Catechins Reduces Body Fat and Cardiovascular Risks. Obesity 2007; 15(6): 1473–83.
- Mombaini E, Jafarirad S and Husain D: The Impact of Green Tea Supplementation on Anthropometric Indices and Inflammatory Cytokines in Women with Polycystic Ovary Syndrome. Phyther Res 2017; (2).
- Kumar R, Bhardwaj P, Thakur S and Kumar S: Tea (Camellia sinensis): A Wonderful Medicinal Herb with Multiple Health Benefits. Chem Sci Rev Lett 2020; 9(34): 454–63.
- Kort DH and Lobo RA: Surgeons. Am J Obstet Gynecol [Internet] 2014; Available from: http://dx.doi.org/10.1016/j.ajog.2014.05.009
- Armanini D, Bonanni G, Mattarello MJ, Fiore C, Sartorato P and Palermo M: Licorice Consumption and Serum Testosterone in Healthy Man. Arman D al Licorice Consum ¼ Exp Clin Endocrinol Diabetes 2003; 341–3.
- Taylor P, Cristina J, Carraro C, Inês M, Dantas DS and Espeschit CR: Flaxseed and human health: reviewing benefits and adverse effects flaxseed and human health: reviewing benefits. Food Rev Int 2012; 37–41.
- Wanegaonkar A, Ayre M, Sayyed N and Jawale R: Unlocking fenugreek’s power PCOS diabetes DR. World Journal of Pharmaceutical Research 2026; 15(6): 385–404.
- Parasuraman S, Thing GS and Dhanaraj SA: Polyherbal formulation: Concept of ayurveda. PHCOG REV 2014; 8(16).
- Patel MG and Prajapati DP: Concept of Polycystic Ovarian Syndrome: Perspectives of Ayurveda and Modern Science IJPPR 2017; 9(10): 1363–72.
- Article R. Review Article ISSN: 3048-5592“. Int J AYURVEDA Gynecol 2025; 2(1): 1–6.
- Williamson EM: Synergy and other interactions in phytomedicines. Phytomedicine 2001; 8(5): 401–9.
- Parasuraman S, Thing GS and Dhanaraj SA: Polyherbal formulation: Concept of ayurveda: Subramani Parasuraman, Polyherbal formulation: Concept of ayurveda Polyherbal formulation: Concept of ayurveda: Subramani Parasuraman. Rev Artic 2014; 4–8.
- Gupta T, Das N and Imran S: The prevention and therapy of osteoporosis : a review on emerging trends from hormonal therapy to synthetic drugs to plant-based bioactives the prevention and therapy of osteoporosis: A Review on. J Diet Suppl ISSN [Internet] 2018; 0211. Available from: https://doi.org/10.1080/19390211.2018.1472715
- Wagner H: Fitoterapia Synergy research : Approaching a new generation of phytopharmaceuticals. Fitoterapia [Internet] 2011; 82(1): 34–7. Available from: http://dx.doi.org/10.1016/j.fitote.2010.11.016
- Kurian A, George S and Thomas B: A Review on Phytochemical Characterization of Kwatha – Ayurvedic Polyherbal Formulation. J Nat Remedies 2021.
- Sankhwar SN, Kumar P, Bagchi M and Rungta M: Safety and Efficacy of Furosap ®, a Patented Trigonella foenum-graecum seed extract, in boosting testosterone level, reproductive health and mood alleviation in male volunteers extract, in boosting testosterone level, reproductive health and mood all. J Am Coll Nutr [Internet] 2021; 0(0): 1–9. Available from: https://doi.org/10.1080/07315724.2021.1978348
- Lakshmi JN, Babu AN, Kiran SSM, Nori LP, Hassan N and Ashames A: Herbs as a source for the treatment of polycystic ovarian syndrome: A Systematic Review. BioTech 2023; 12(4): 1–21.
- Arentz S, Smith CA, Abbott JA and Bensoussan A: A survey of the use of complementary medicine by a self-selected community group of Australian women with polycystic ovary syndrome. Arentz al BMC Complement Altern Med 2014; 14: 1–6.
- Talaat B, Mohamed I and Ammar M: The added value of cinnamon to metformin in controlling symptoms of polycystic ovary syndrome, a randomized controlled trial. Middle East Fertil Soc J [Internet] 2018; 3–8. Available from: https://doi.org/10.1016/j.mefs.2018.03.005
- Colonetti L, José A, Reynaud I, Bisognin L, Inês M and Colonetti T: Green tea promotes weight loss in women with polycystic ovary syndrome : Systematic review and meta-analysis. Nutr Res 2022; 104: 1–9.
- Liao W, Su C, Lee M, Li C, Lin C and Chiang J: Integrative Chinese herbal medicine therapy reduced the risk of type 2 diabetes mellitus in patients with polycystic ovary syndrome : A nationwide matched cohort study. J Ethnopharmacol [Internet] 2019; 243(2): 112091. Available from: https://doi.org/10.1016/j.jep.2019.112091
- Sharifi M, Saber A, Moludi J, Salimi Y and Jahan-Mihan A: The effects of portfolio moderate-carbohydrate and ketogenic diets on anthropometric indices, metabolic status, and hormonal levels in overweight or obese women with polycystic ovary syndrome: a randomized controlled trial. Vol. 23, Nutrition Journal 2024; 1–32.
- Yarak S, Brasil Parada MOA, Bagatin E, Talarico Filho S and Hassun KM: Hyperandrogenism and skin: Polycystic ovary syndrome and peripheral insulin resistance. An Bras Dermatol 2005; 80(4): 395–410.
- Walters KA, Allan CM and Handelsman DJ: Minireview Rodent Models for Human Polycystic Ovary Syndrome 1. Biol Reprod 2012; 86(2): 1–12.
- Legro RS, Dodson WC, Kris-etherton PM, Kunselman AR, Stetter CM and Williams NI: Randomized Controlled Trial of Preconception Interventions in Infertile Women with Polycystic Ovary Syndrome. J Clin Endocrinol Metab 2015; (10): 1–11.
- Tang T, Jm, Lord, Rj N, Yasmin E and Ah B: pioglitazone, D-chiro-inositol) for women with polycystic ovary syndrome, oligo amenorrhoea and subfertility (Review). TheCochrane Libr 2012; (5).
- Garad RM and Teede HJ: ScienceDirect Polycystic ovary syndrome : improving policies, awareness, and clinical care. Curr Opin Endocr Metab Res [Internet] 2020; 12: 112–8. Available from: https://doi.org/10.1016/j.coemr.2020.04.007
- Legro RS, Dodson WC, Kunselman AR, Stetter CM, Kris-etherton PM and Ph D: Benefit of Delayed Fertility Therapy with Preconception Weight Loss over Immediate Therapy in Obese Women with PCOS. J Clin Endocrinol Metab 2016; (5): 1–9.
- Huang X, Wang P, Tal R, Lv F, Li Y and Zhang X: A systematic review and meta-analysis of metformin among patients with polycystic ovary syndrome undergoing assisted reproductive technology procedures. Int J Gynecol Obstet [Internet] 2015; Available from: http://dx.doi.org/10.1016/j.ijgo.2015.04.046
- Michałowska J and Miller-kasprzak E: Incretin Hormones in Obesity and Related Cardiometabolic Disorders: The Clinical Perspective Nutrients 2021.
- Review AS. Susan Arentz, Jennifer Hunter and Gary Deed: J Altern Complement Med 2020; 26(7): 571–91.
- Kwon Y, Kim M, Kim Y, Jung HS and Jeoung D: Exosomal MicroRNAs as Mediators of Cellular Interactions between Cancer Cells and Macrophages. Front Immuno 2020; 11(6): 1–14.
- Complimentary Copy.
- Balkrishna A, Sharma N, Diwakar S, Parveen R, Kukreti A and Trivedi B: Review Article Integrated Management of Cortisol : A Multidimensional Perspective. Futur Integr Med 2026 [Internet] 2026; 000(000): 1–23. Available from: https://www.doi.org/10.14218/FIM.2025.00062
- Moore E, Patanwala I, Jafari A, Davies IG, Kirwan RP and Newson L: A systematic review and meta-Analysis of randomized controlled trials to evaluate plant-based omega-3 polyunsaturated fatty acids in nonalcoholic fatty liver disease patient biomarkers and parameters. Nutr Rev 2024; 82(2): 143–65.
- Reddy VN, Ahmed MF and Anjum A: Peer Reviewed Journal, ISSN 2581-7795. Peer Rev J 9(3): 153–68.
- PVDB and PVDB: Cardiovascular Toxicities of Herbal Products : An Overview of Selected Compounds. Toxicol Herb Prod 2017; 363–83.
- Seamon MJ, Clauson KA, Ephedra, Yesterday, Dshea and Tomorrow: A ten year perspective on the dietary supplement health and education Act of 1994. J Herb Pharmacother 1994; 5(3): 67–86.
- Peschel W and Monedero B: Harmonised European Standards as a Basis for the Safe Use of Herbal Medicinal Products and Their Marketing Authorisation in European Union Member States. Pharm Med 2018; 40290.
- Zhang M, Wang C, Zhang R, Chen Y, Zhang C and Heidi H: Comparison of the guidelines on good agricultural and collection practices in herbal medicine of the European Union, China, the WHO, and the United States of America. Pharmacol Res [Internet]. 2021; 167(3): 105533. Available from: https://doi.org/10.1016/j.phrs.2021.105533
- Izzo AA and Ernst E: Interactions between herbal medicines and prescribed drugs an updated systematic review. Drugs 2009; 69(13): 1777–98.
- Posadzki P, Lee MS, Moon TW, Choi TY, Park TY and Ernst E: Maturitas Prevalence of complementary and alternative medicine (CAM) use by menopausal women: A systematic review of surveys. Maturitas [Internet] 2013; 75(1): 34–43. Available from: http://dx.doi.org/10.1016/j.maturitas.2013.02.005
- Quality control methods for herbal materials. world health organization 1998.
- Singh RK, Sharma K, Gupta MP, Ravikant, Rajpurohit MS and Saxena V: Exploring Nanotechnology with Traditional Herbal Pharmacology: Nano Carrier-Based Phytochemical Delivery in PCOS Treatment. Nanotechnol NextGen from Treat to Transform Polycystic Ovary Syndr 2025; 49–78.
- Jolanda van Keizerswaard, Alexandra L. Dietz de Loos, Yvonne V. Louwers and Joop S. E. Laven: Changes in individual polycystic ovary syndrome phenotypical characteristics over time: a long-term follow-up study. Fertil Steril [Internet] 2003; 117(5): 1059–66. Available from: https://doi.org/10.1016/j.fertnstert.2022.01.014
- Azziz R, Tarlatzis R, Dunaif A, Ibanez L, Pugeat M and Taylor A: Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Rotterdam PCOS Consens Work 2004; 81(1): 19–25.
- Gurib-Fakim A: Novel plant bioresources : applications in food, medicine and cosmetics. In: 2014, editor. 1st ed. John Wiley & Sons, Ltd Registered 2014.
How to cite this article:
Lone MS, Singh RK, Sharma T and Kushwaha S: “Biomechanical alterations in women with polycystic ovary syndrome: linking lumbopelvic alignment”. Int J Pharmacognosy 2026; 13(5): 368-91. doi link: http://dx.doi.org/10.13040/IJPSR.0975-8232.IJP.13(5).368-91.
This Journal licensed under a Creative Commons Attribution-Non-commercial-Share Alike 3.0 Unported License.
Article Information
2
368-391
653 KB
121
English
IJP
Mohammad Sadam Lone, Ranjan Kumar Singh *, Tanya Sharma and Satpal Kushwaha
Department of Pharmacy, Mewar University, Gangrar, Chittorgarh, Rajasthan, India.
rxsingh41800557@gmail.com
19 April 2026
03 May 2026
09 May 2026
10.13040/IJPSR.0975-8232.IJP.13(5).368-91
15 May 2026