


AN OVERVIEW ON CAMELLIA SINENSIS AS ANTIASTHMATIC
HTML Full TextAN OVERVIEW ON CAMELLIA SINENSIS AS ANTIASTHMATIC
Divya Bhandari, Gaurav Joshi and Prabhjot Kaur
UIPS, Chandigarh University 1, Gharuan, Mohali, Punjab, India.
ABSTRACT: The present era aims to use medicinal plants and their constituents to treat various diseases. The synthetic drugs available in the market are associated with various side effects and follow a tedious and time-consuming process to synthesize. Natural drugs are safe and possess a large therapeutic window, thus gaining interest in the present scenario. These natural drugs are lacking in terms of their receptor action, so the present scenario aims to extract the active constituents of herbal drugs and study their profile aiming at a particular disease. In the present review, we presented the antiasthmatic potential of caffeine (extracted from tea leaves) by studying its effect on adenosine receptors. Our main aim is to study the active constituent present in a specific part of the plant to be extracted and used specifically for a specific receptor instead of the whole plant.
Keywords: Antiasthmatic, Adenosine receptors, Camellia sinensis, Asthma, A2A receptor
INTRODUCTION: Disease cannot be defined as the opposite of health as there is no single definition to define health; thus, defining disease is challenging. As defined by WHO (1946), health is a state of complete physical, mental and social well-being, not merely the absence of disease or infirmity. In the present scenario, a rise in the number of infectious diseases can be observed especially related to the respiratory system. Asthma is one of the respiratory system's leading diseases and affects about 50-60% of world's population. Asthma can be defined as a chronic, obstructive and inflammatory disorder of pulmonary airways associated with airways inflammation and hyperresponsiveness due to some stimulus resulting in constriction of bronchioles 1.
Asthma is considered one of the chronic and serious allergic diseases. The Global Strategy for Asthma Management and prevention defines asthma as “a chronic inflammatory disorder of the airways in which many cells and cellular elements play a role.” The chronic allergy and inflammation result in repeated episodes of sneezing, breathlessness, chest tightness and coughing. These episodes are more prevalent at night or in the early morning. These episodes result in an obstruction of airways which is usually reversible spontaneously or with treatment.
The airways obstruction is due to muscle contraction or hypersecretion resulting in airway tissue reactions 2. A number of drug management groups, such as the National Institutes of Health (USA), the Global Initiative for Asthma (GINA), and the Japanese Society of Allergology (JSA) have given various prevention and management guidelines for asthma prevention 3-7. These guidelines are both for treatment and prevention in adults and children, but complete remission is difficult 2.
India reports 15-20 million asthmatic patients, in which almost 15% are between the age of 5-10 years. There are a number of factors that play an important role in the occurrence of this disease. These include gender, age, family history of asthma, atopy history, lower socioeconomic status, and urbanization 8. The common cause of sneezing in rural areas is usually smoking, intake of paracetamol, air pollution due to traffic, and cat exposure 9. The most accepted treatment of asthma includes the use of Bronchodilators and corticosteroids. Among herbal drugs, caffeine, an ingredient of Tea leaves, acts as a bronchodilator to provide symptomatic relief.
Caffeine: Caffeine is usually found as one of the ingredient in coffee, tea, cocoa and cold drinks. The term Caffeinated drinks is used for drinks containing caffeine. Caffeine on a temporary basis makes one feel more energetic, awake, and focused by stimulating CNS. The major source of caffeine is Tea leaves, i.e., Camellia sinensis. Each type of tea comes from a different species of C. sinensis.
Camellia Sinensis: C. sinensis is known by different names, which varies from country to country and region to region. Following is the list of few common names of plant C. sinensis.
Biological Source: Caffeine is obtained from the leaves of Camellia sinensis of family Theaceae- Tea family, Order-Theales, Subclass-Dilleniidae, Class-Magnoliopsida- Dicotyledons, Division-Magnoliophyta- Flowering plants, and subdivision-Spermatophyta- Seed plants.

FIG. 1: LEAVES OF CAMELLIA SINENSIS
Morphology of C. sinensis: Camellia sinensis, a plant of the Araceae family found as an evergreen tree or a shrub that usually grows upto a height of 10-15 meter in the wild species; when cultivated, it grows around 0.6-1.5 meters.
The leaves of this plant are green in colour Fig. 1, short-stalked, alternate, lanceolate, serrate margin, glabrous or pubescent beneath, which varies from 5-30 cm in length and 4 cm wide. As the leaves mature, they turn bright green in colour and leathery in touch. The flowers are white in color, fragrant with around 2.5-4 cm diameter, and usually found in clusters of 2-4 10. The fruit part is flat, smooth, round 3 cell capsule and almost of size of small nut 11.
Varieties of C. sinensis: The plant Camellia sinensis is a native of China and grows in cold weather and at altitudes. It is usually found in two main varieties yielding different types of tea with different characteristics, such as white tea and green tea. Green tea is not oxidized and is usually pan-fried to prevent it from oxidation 12. Camellia sinensis as samica, another variety is known as Assam or Indian tea and is native to the Northern region of Assam. It is more tropical than the Chinese variety and grows larger due to warm temperatures and heavy rainfall.
It includes Black tea (Red tea) and Oolong tea. Black tea is more oxidized during processing than Oolong tea thus tastes strong.
Origin: The tea plant was discovered by accident around 2737 B.C.E. An emperor of that time was boiling water in his garden and a leaf of C. sinensis tree fell into that pot. This combination resulted in a drink that forced him to do further research on that plant, including medicinal and palatable properties.
Cultivation: The plant C. sinensis usually grows in tropical climates, but the Chinese variety can even grow in cooler and higher altitude climates. In US, tea usually grows in the subtropical region of the southeast in Hawaii and in the cool climate of the Pacific Northwest. Some gardeners grow this plant as a shrub resulting in a small tree, but some cultivators believe that the taller the plant, the larger the root structure, and the more nutritious and flavourful the tea is. This plant usually grows in well-drained sandy soil and should be harvested after three years of age.
Harvesting: Harvesting of tea leaves is done by hand as only top leaves are required to be plucked. During harvesting, only young top leaves are plucked having small tips. While plucking a small portion of the stem having 2-5 leaves and tip is included, this is known as ‘golden flush’. During warm months, the plant grows strong so tea is harvested during this month. So, there are only 4 months of harvesting in northern regions, while in tropical areas, harvesting can be done up to 8 months.
Composition of Tea: Tea usually contains thousands of bioactive compounds such as carbohydrates, polyphenols, flavonoids, amino acids, and volatile substances, among which 1/3rd constitute polyphenols. Polyphenols contain benzene rings bonded together by -OH groups. Polyphenols include flavonoids, non-flavonoids, and alkaloids, but only flavonoids 13 and alkaloids are present in tea. These are secondary metabolites obtained by a reaction of cinnamic acid with three malonyl CoA and acts as a defense mechanism against insects and animals. The major flavonoids present are flavanols, anthocyanidins, flavones, flavanones and isoflavonoids 14, responsible for the health claim of tea possessing antioxidant properties. The alkaloids present are caffeine, theobromine, and theophylline, which add bitterness to tea. Amino acid, along with caffeine, helps in improving memory and learning. The amount of caffeine found in various varieties of tea is given in Table 1.
TABLE 1: GENERALLY ACCEPTED AMOUNT OF CAFFEINE IN TEA
| Type | 6-8 oz. cup | Water temp | Steeping time | Amount of Caffeine |
| Coffee | 1 tsp | To 212 | NA | 120mg |
| White | 1 tsp | 175-1851 | 2-3 | 15 mg |
| Green | 1 tsp | 185 | 2-3 | 25 mg |
| Oolong | 1 tbsp | 206 | 3-6 | 30 mg |
| Black | 1 tsp | 185-212 | 3-5 | 40 mg |
| Pu-erh | 1 tbsp | 195-206 | 5-7 | 30-40 mg |
| Chai | Receipe | 212 | 7-10 | 40 mg |
Mechanism of Action of Caffeine: Caffeine (1, 3, 7-trimethylxanthine), a purine alkaloid, is reported as the most widely used bronchodilator drug in the world. A large population reports regular use of caffeine and caffeine-containing beverages and foods 15. The daily intake of caffeine in the USA and Canada is reported to be 200-250 mg/person per day, while in Nordic countries and Great Britain, it is 300-400 mg/person per day 15, 16. Caffeine is absorbed easily from GIT and distribute in all body fluids. The metabolism of caffeine includes complex series of reactions and a peak plasma concentration within 15-20 min of oral ingestion 17-21. A number of mechanisms are reported to explain the action of caffeine but most accepted is its antagonism at adenosine receptors (A1, A2A, A2B and A3) 22-24 in CNS25-27 and in CVS 28-30 due to its structural similarity with adenosine Fig. 2.
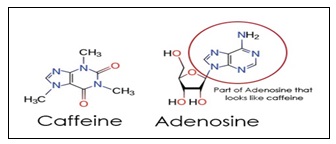
FIG. 2: CAFFEINE AND ADENOSINE
Among subtypes of adenosine A1 and A3 types inhibit adenyl cyclase while A2A and A2B stimulate increasing cAMP production 17.
Thus, A2A receptors existing in various WBC’s, mast cells, smooth muscles 31-32 and platelets, on activation, are associated with the vasodilation of coronary and also peripheral vasodilation 33-34 neo-angiogenesis 35 and also affect the synthesis of cytokines from the cells of the immune system and also from the cells involved in inflammation 36. The studies on humans suggest that excess caffeine consumption may result in an antithrombic effect and prevent aggregation of platelets due to A2A adenosine receptor upregulation 37-39. The platelet associated effect of caffeine depends on how much caffeine is taken for how long the duration of time 38, 39. The exact link between caffeine and its anti-inflammatory effect is misleading. The study on selective agonists can better explain the anti-inflammatory effect, and subsequently, antagonists increasing inflammation and may result in tissue damage 40-42. Further studies report that caffeine is also effective in vitro in suppressing TNF production, a cytokine in human blood 43. The field of interest in this area is to study further the anti-inflammatory effect of caffeine in various humans 43-44.
CONCLUSION: Of all the reported diseases and disorders, asthma is a leading serious disorder affecting a large population of the world. Among reported cases of asthma from all age groups, the highest percentage is of children and adults till 18 years of age. India has approximately 15-20 million asthmatic patients while countries are sounding well medically like USA had made a database of their citizens developing allergy (asthma) from plants. This database includes the pollination time of plants, thus reflecting measures taken by a country towards the health maintenance of its citizens. However, the contribution of synthetic medicines for the treatment of such disorders is associated with harmful side effects. Over the past few decades, the serious realization of problems associated with synthetic medicines has gained attention towards herbs and natural products. These natural therapies are easily available, nut and economical, and free from any side effect. A lot of work is still required on tea to determine its actual potential for human use. Clinical trials are mandatory to collect data of its active constituents, and also there is a need for the development of the best-suited dosage form and effective route of administration. Still, more research is required in this field to study the underlying properties of tea, the mechanism of action of caffeine, and its role in asthma.
ACKNOWLEDGEMENT: Authors would like to thank Chandigarh University for giving facilities for data collection.
CONFLICTS OF INTEREST: University Institute of Pharma Sciences.
REFERENCES:
- O'Byrne PM: Global guidelines for asthma management: summary of the current status and future challenges. Pol Arch Med Wewn 2010; 120: 511-17.
- Hoeksema LJ, Bazzy A, Lemotan EA, Edmonds DE, Ramirez-Garnica G and Shiffman RN: Accuracy of a computerized clinical decision-support system for asthma assessment and management. J Am Med Inform Assoc 2011; 18: 243-50.
- Moore WC and Pascual RM: Update in asthma 2009. Am J Respir Crit Care Med 2010; 181: 1181-87.
- Dahlén SE, Dahlén B and Drazen JM: Asthma treatment guidelines meet the real world. N Engl J Med 2011; 364: 1769-70.
- Ohta K, Yamaguchi M, Akiyama K, Adachi M, Ichinose M and Takahashi K: Japanese guideline for adult asthma. Allergol Int 2011; 60: 115-45.
- Sears MR, Greene JM and Willan AR: A longitudinal, population-based, cohort study of childhood asthma followed to adulthood. N Engl J Med 2003; 349: 1414-22.
- Haland G, Carlsen KC and Sandvik L: Reduced lung function at birth and the risk of asthma at 10 years of age. N Engl J Med 2006; 355: 1682-89.
- Corbin JD and Francis SH: Pharmacology of phosphodiesterase-5 inhibitors. Int J Clin Pract 2002; 56: 453-59.
- Rotella DP: Phosphodiesterase-5 inhibitors: current status and potential applications. Nat Rev Drug Discov 2002; 1: 674-82.
- Ross IA: Tea common names and its uses. In Medicinal Plants of the World 2005; 3: 1-19
- Biswas KP: Description of tea plant. In Encyclopaedia of Medicinal Plants. New Delhi: Dominant Publishers and Distributors 2006; 964-66.
- Cabrera C, Artacho R and Gimenez R: Beneficial effects of green tea- A Review. J Am Coll Surg 2006; 25: 79-99.
- Sumpio BE, CordovaC, Berke-Schlessel DW, Qin F and Chen QH: Green tea, the “Asian Paradox”, and cardiovascular disease. J Am Coll Surg 2006; 202: 813-20.
- Yilmaz, Y: Novel uses of catechins in food. Trends. Food Sci Technol 2006; 17: 64-71.
- Fredholm BB, Battig K, Holmen J, Nehlig A and Zvartau EE: Actions of caffeine in the brain with special reference to factors that contribute to its widespread use. Pharmacol Rev 1999; 51; 83-33.
- Mandel HG: Update on caffeine consumption, disposition and action. Food Chem Toxicol 2002; 40; 1231-34
- Arnaud MJ: Metabolism of 1,3,7-trimethyldihydrouric acid in the rat: new metabolic pathway of caffeine. Experientia 1976; 32: 1238-40.
- Levitt DG: Quantitation of small intestinal permeability during normal human drug absorption. BMC Pharmacol Toxicol 2013; 14: 34.
- Arnaud MJ: Pharmacokinetics and metabolism of natural methylxanthines in animal and man. Handb Exp Pharmacol 2011; 200: 33-91.
- Liguori A, Hughes JR and Grass JA: Absorption and subjective effects of caffeine from coffee, cola and capsules. Pharmacol Biochem Behav 1997; 58: 721-26.
- Skinner TL, Jenkins DG, Leveritt MD, McGorm A, Bolam KA and Coombes JS: Factors influencing serum caffeine concentrations following caffeine ingestion. Journal of Science and Medicine in Sport 2014; 17: 516-20.
- Fredholm BB, Ijzerman AP, Jacobson KA, Klotz KN and Linden J: International Union of Pharmacology. XXV. Nomenclature and classification of adenosine receptors. Pharmacol Rev 2001; 50: 527-52.
- Thong FSL and Graham TE: The putative roles of adenosine in insulin and exercise mediated regulation of glucose transport and glycogen metabolism in skeletal muscle. Can J Appl Physiol 2002; 27; 152-78.
- Graham TE: Caffeine and exercise: metabolism, endurance and performance. Sports Med 2001; 31: 785-07.
- Alsene K, Deckert J S and Wit PH: Association between A2A receptor gene polymorphisms and caffeine induced anxiety. Neuropsychopharmacol 2003; 2: 1694-02.
- Fredholm BB: Adenosine, adenosine receptors and the actions of caffeine. Pharmacol Toxicol 1998; 76: 93-01.
- Ross GW, Abbott RD, Petrovitch H, White LR and Tanner CM: Relationship between caffeine intake and Parkinson disease. JAMA 2000; 284: 1378-79.
- White PJ and Nguyen TT: Chronic caffeine treatment causes changes in cardiac adenosine receptor function in rats. Pharmacol 2000; 65: 129-35.
- Aqel RA, Zoghbi GJ and Trimm JR: Effect of caffeine administered intravenously on intracoronary-administered adenosine-induced coronary hemodynamics in patients with coronary artery disease. American Journal of Cardiology 2004; 93:434-46
- Myers MC: Effect of caffeine on blood pressure beyond the laboratory. Hypertension 2004; 43; 724-25
- Varani K, Gessi S, Dionisotti S, Ongini E and Borea PA: [3H]-SCH 58261 labelling of functional A2A adenosinereceptors in human neutrophil membranes. Br J Pharmacol 2008; 123: 1723-31
- Gessi S, Varani K, Merighi S, Ongini E and Borea PA: A2A adenosine receptors in human peripheral blood cells. Br J Pharmacol 2000; 129: 2–11.
- Belardinelli L, Shryock JC, Snowdy S, Zhang Y, Monopoli A and Lozza G: The A2A adenosine receptor mediates coronary vasodilation. Journal of Pharmacology and Experimental Therapeutics 1998; 284:1066-73.
- Grobbee DE, Rimm EB, Giovannucci E, Colditz G, Stampfer M and Willet W: Coffee, caffeine, and cardio vascular disease in men. The New England Journal of Medicine 1990; 323: 1026-32.
- Sexl V, Mancusi H, Holler C, Gloria ME, Schutz W and Freissmuth M: Stimulation of the mitogen-activated protein kinase via the A2A adenosine receptor in primary humanendothelial cells. J Biol Chem 1997; 272: 5792-99
- Varani K, Laghi-Pasini F, Camurri A, Capecchi PL, Maccherini M and Diciolla F: Changes of peripheral A2Aadenosine receptors in chronic heart failure and cardiac transplantation. FASEB J 2003; 17: 280-82
- Biaggioni I, Paul S, Puckett A and Arzubiaga C: Caffeine and theophylline as adenosine receptor antagonists inhumans. J Pharmacol Exp Ther 1991; 258: 588-93
- Varani K, Portaluppi F, Merighi S, Ongini E, Belardinelli L and Borea PA: Caffeine alters A2A adenosine receptorsand their function in human platelets. Circulation 1999; 99: 2499-02
- Varani K, Portaluppi F, Gessi S, Merighi S, Ongini E and Belardinelli L: Dose and time effects of caffeine intakeon human platelet adenosine A2A receptors: functional and biochemical aspects. Circulation 2000; 102: 285-89
- Montesinos MC, Yap JS, Desai A, Posadas I, McCrary CT and Cronstein BN: Reversal of the anti-inflammatory effects of methotrexate by the nonselective adenosine receptor antagonists theophylline and caffeine: evidence that the anti-inflammatory effects of methotrexate are mediated via multipleadenosine receptors in rat adjuvant arthritis. Arthritis Rheum 2000; 43: 663-65.
- Thiel M, Caldwell, CC and Sitkovsky MV: The critical role of adenosine A2A receptors in downregulation of inflammation and immunity in the pathogenesis of infection diseases. Microbes Infect 2003; 5: 515-26.
- Gomez G, Sitkovsy and MV: Targeting G protein-coupled A2A adenosine receptors to engineer inflammation in-vivo. J Biochem Cell Biol 2003; 35: 410-14
- Horrigan LA, Kelly JP and Connor TJ: Caffeine suppresses TNF-a production via activation of the cyclic AMP/protein kinase a pathway. Intern Immunopharm 2004; 4: 1409-17.
- Jafari M and Rabbani A: Studies on the mechanism of caffeine action in alveolar macrophages: caffeine elevatescyclic adenosine monophosphate level and prostaglandin synthesis. Metabolism 2004; 253: 687-92.
How to cite this article:
Bhandari DD, Joshi G and Kaur P: An overview on Camellia sinensis as antiasthmatic. Int J Pharmacognosy 2020; 8(7): 278-82. doi link: http://dx.doi.org/10.13040/IJPSR.0975-8232.IJP.8(7).278-82.
This Journal licensed under a Creative Commons Attribution-Non-commercial-Share Alike 3.0 Unported License.