MALARIA AND ANTIMALARIAL ACTIVITY OF MEDICINAL PLANTS: A REVIEW
HTML Full TextMALARIA AND ANTIMALARIAL ACTIVITY OF MEDICINAL PLANTS: A REVIEW
Shilpa S. Raut
K. K. Wagh College of Pharmacy, Amrutdham, Nashik - 422003, Maharashtra, India.
ABSTRACT: Natural compounds have already contributed to the discovery of new anti-malarial drugs. Atovaquone, artemisinin and its semi-synthetic derivatives as well as clindamycin, erythromycin, azithromycin, chlortetracycline, tetracycline, oxytetracycline and doxycycline, are noteworthy examples of the varied contribution of natural products for the development of effective anti-malarial drugs, particularly valuable for the treatment of chloroquine-resistant parasites. To avoid side effects and the resistance developed by the synthetic drug natural drug preffered. However, in many cases good activity and selectivity were observed. Most importantly, several compounds containing unique structural composition have been isolated and characterized. In the present review, a number of potential anti-malarial plants explored have been brought out, and a number of leads suggested on the basis of their anti-malarial activities. Thus, it provides guidance for areas of further research on potential plant resources that could be sources of compounds with therapeutic properties for the treatment of malaria. Some of the plants were investigated for anti-malarial activities, and their efficacy, toxicity, and safety aspects still need to be studied.
| Keywords: |
Malaria, Anti-malarial, Artemisinin, Plasmodium vivax, Plasmodium falciparum
INTRODUCTION: Malaria had its origins in the jungles of Africa. Malaria always has and will remain as Public Health Problem in Maharashtra, Jeopardizing the development of State on account of heavy morbidity and mortality. Thus economic loss was enormous and estimated to run into Hundreds of Crores of Rupees every year. Malaria manifests as fever, chills, prostration, and anemia. A severe form of the disease may lead to delirium, metabolic acidosis, cerebral malaria, multi-organ system failure, coma, and death. Malaria is a febrile disease caused by the blood parasite called Plasmodium transmitted by the bite of an infected female anopheles mosquito.
Malaria is the most common disease in Africa. It is also the cause of death among young children and a significant cause of miscarriages among pregnant mothers. Humans have always coexisted with parasites. The infectious disease malaria is caused by the protozoan parasite of the genus Plasmodium, and it is one of the most dangerous diseases infecting human populations. Approximately 300 - 500 million people are infected annually, and 1.5 - 2.7 million lives are lost to malaria each year.
Four species of the Sporozoa are recognized as etiological agents in human malaria Plasmodium vivax, Plasmodium ovale, Plasmodium malariae, and Plasmodium falciparum. P. falciparum is the most dangerous with the highest morbidity rates, and generally is the only species that may cause death in humans. The resistance of the malaria parasite to drugs and the resistance of the mosquitoes to insecticides has resulted in the resurgence of malaria in many parts of the world.
There is a pressing need for vaccines and new drugs 1, 2.
The Different Species of Malaria Causing Parasite: There are four species of Plasmodium that infect humans.
Plasmodium Vivax (Tertian): It is the most common species in the World. It is the largest of the malaria parasites found in humans. The length of its asexual cycle is 48 h. Relapses are common in vivax malaria due to the emergence of new blood forms from maturing secondary liver schizonts. In tropical areas, relapses may arise within three to four months of the primary attack, while in subtropical areas, relapses occur only after nine months or more.
Plasmodium Ovale (Tertian): It is a relatively rare species with a frequency of less than 5%. It may sometimes be confused with P. vivax. The length of its asexual cycle is 48 h. Relapses occur as in P. vivax, but the disease tends to be more chronic.
Plasmodium Malariae (Quartan): It is a less common species whose length of its asexual cycle is 72 h. P. malaria is associated with quartan malaria.
Plasmodium Falciparum (Sub-Tertian): It is the commonest species in Africa, and it accounts for 95 - 98% of all malaria infections. It is responsible for severe illness cerebral malaria, and other complications and may cause death. The length of the asexual cycle is about 48 h. Fever is produced when the schizonts are mature i.e. at 48 h interval. Sub-tertian means that diurnal periodicity is common. The liver stage of development takes about 14 days.
The Malaria Life Cycle: The Malaria parasite lifecycle begins when an infected adult female Anopheles mosquito bites a human being to feed on his or her blood. As it feeds on this blood, it releases malaria sporozoites (parasites) into the blood stream of the host (human being). This is the infective bite. Once the parasites enter the human blood stream they move quickly to the liver cells where they develop and multiply (schizogony). The infected liver cells rapture and release numerous merozoites into the blood, which invade red blood cells (RBCs). This stage takes 9-14 days. Within the RBCs, the parasites develop from “rings” into blood schizonts. The schizonts then rupture the RBCs releasing numerous merozoites that invade new RBCs. When the infected red blood cells rapture, this process initiates the chills and fever, which are characteristic of Malaria. Indeed, the peaks of fever experienced during malaria coincide with the release into the blood circulation of malaria parasites (merozoites) from raptured RBCs. The period between the infective bite and the onset of symptoms (i.e., fever chills, etc.) is called the incubation period of malaria. As we mentioned earlier, the incubation period is usually 7-14 days but may be shorter as in P. falciparum or longer in the case of P. vivax and P. malariae. See Fig. 1 for an illustration of the cycle of malaria 1, 2.
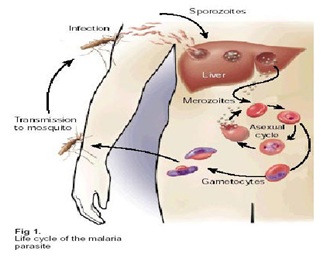
FIG. 1: LIFE CYCLE OF HUMAN MALARIA PARASITE
Pathophysiology of Malaria: The life cycle of malaria includes the vector stages. Malaria causes metabolic and neurological complications. While anemia hypoglycemia and renal failure require urgent treatment, Planche and Krishna found that cerebral malaria and lactic acidosis were independent predictors of poor outcomes. The metabolic changes that are important in severe malaria are acidosis, hyperlactatemia, and respiratory distress. The biggest culprit appears to be increased anaerobic glycolysis due to microvascular obstruction. Interestingly, serum lactate levels were found to be higher in malaria than in sepsis, indicating impaired oxygen delivery. Dichloroacetate has been shown to safely lower blood lactate concentration, but more research is needed to assess its capacity to reduce mortality in cases of severe malaria.
In addition to the hypoglycemia induced by patients who are administered quinine (due to increased insulin secretion), hypoglycemia can also be a result of the demands of anaerobic glycolysis.
Every patient should be assessed for hypoglycemia on admission, and inpatient care must include regular monitoring of blood glucose levels. Malaria is defined as “an unrousable coma with asexual P. falciparum infection at least 30 min after a convulsion, when hypoglycemia has been excluded and without interference by sedative drugs or other confounding variables.” However, the authors cited studies that suggest that impaired consciousness, rather than coma, maybe a more accurate predictor of death. Originally, it was believed that cerebral edema resulting from increased capillary permeability, was the cause of cerebral malaria 3.
Principles of Treatment: Treatment of malaria depends on the following factors:
A. Type of infection.
B. Severity of infection.
C. Status of the host.
D. Associated conditions/diseases.
A. Type of Infection: Treatment obviously depends on the type of infection. Patients with P. falciparum malaria should be evaluated thoroughly in view of the potential seriousness of the disease and the possibility of resistance to anti-malarial drugs.
vivax: Only Chloroquine 25 mg/kg + Primaquine for 14 days.
falciparum: Treat depending on severity & sensitivity. Primaquine as gametocytocidal, is a must to prevent spread.
Mixed Infections: Blood schizonticides as for P. falciparum and Primaquine as for P. vivax.
B. Severity of Infection: All patients with malaria should be carefully and thoroughly assessed for complications of malaria. Acute, life-threatening complications occur only in P. falciparum malaria. Malaria is probably the only disease of its kind that can be easily treated in just 3 days, yet if the diagnosis and proper treatment are delayed, it can kill the patient very quickly and easily.
- All cases of severe malaria should be presumed to have falciparum malaria.
- If there is any uncertainty about the drug sensitivity of the parasite, it is safer to treat these cases as chloroquine-resistant malaria with drugs like quinine or artemisinin.
- All cases of severe malaria should be admitted to the hospital for proper evaluation, treatment, and monitoring.
- All cases of severe malaria should be treated with injectable anti-malarial (chloroquine, quinine, and artemisinin) so as to ensure adequate absorption and plasma drug levels. It is better to use two blood schizonticidal drugs, one fast-acting and another slow-acting, to ensure complete treatment. Newer drugs available for only oral administration (g. Mefloquine, Halofantrine) should be avoided.
- All associated conditions should be carefully assessed and treated.
C. Status of the Host: Treatment of malaria is also dependent on host factors.
- Patient's age and weight should be recorded so as to administer adequate doses of anti-malarial drugs.
- Functional capacity- independent, dependent, bed ridden All patients with severe prostration and who are looking ill should be admitted to a hospital and monitored.
- Patients with nausea and vomiting should be given anti-emetic drugs to ensure adequate treatment. While high-grade fever frequently stimulates vomiting, this may be further aggravated by anti-malarial drugs. Therefore, it is better to avoid the administration of oral anti-malarial at the height of fever. One can wait for the fever to subside before taking the drugs. If the patient vomits within one hour of taking the anti-malarial drugs, the same should be re-administered. In case of persistent vomiting, the patient should be admitted, and vomiting should be controlled with parenteral antiemetics. Parenteral antimalarials are needed only in cases of severe malaria or uncontrolled vomiting.
- Adequate hydration should be ensured.
D. Associated Conditions/Diseases: Treatment of malaria may have to be modified due to certain associated conditions/diseases. Therefore, all such should be carefully assessed before starting the patient on anti-malarial treatment.
Pregnancy: Treatment of malaria in pregnancy may prove to be difficult due to contraindication for the use of certain anti-malarial. Chloroquine can be used safely in all trimesters of pregnancy. Artemisinin is not shown to have any deleterious effects on the fetus in animal studies and, therefore, can be considered if the situation demands. Quinine can be used in pregnancy, but one should be watchful about hypoglycemia. Whereas Mefloquine is contraindicated in the first trimester of pregnancy, pyrimethamine/ sulphadoxine is contraindicated in the first and last trimesters. Halofantrine, tetracycline, and doxycycline are absolutely contraindicated in pregnancy. Primaquine is also contraindicated in pregnancy, and therefore pregnant women with P. vivax malaria should be started on 500 mg of chloroquine weekly as suppressive chemoprophylaxis against relapse of malaria.
Epilepsy: Malaria, as well as anti malarials, can trigger convulsions. Mefloquine is better avoided in these patients.
Cardiac Disease: High-grade fever of malaria can exacerbate left ventricular failure and, therefore, in all such patients’ energetic management of malaria is called for. Fever should be controlled with antipyretics and tepid sponging. Chloroquine, artemisinin, pyrimethamine/sulphadoxine, tetracyclines, and primaquine can be safely used in these patients. Quinine can also be used carefully. Mefloquine and halofantrine are better avoided in patients with known cardiac illness.
Hepatic Insufficiency: None of the anti-malarial drugs have any direct hepatotoxic effect. However, chloroquine is not advisable in patients with severe hepatic insufficiency.
Renal Failure: The initial dose of anti-malarial drugs need not be reduced in patients with renal failure. However, if the patient requires parenteral anti-malarial even after three days and Continues to be sick, then the dose can be reduced by one third to half of the usual dose. See renal disease and malaria.
Dermatitis: Concomitant use of chloroquine with gold salts and phenylbutazone should be avoided because all three can cause dermatitis 7, 8.
Modes of Treatment: Two important concepts in the treatment of malaria are suppressive and radical treatments.
Suppressive Treatment: The symptoms of malaria can be alleviated by suppressing the erythrocytic stage of parasitic development. Suppressive therapy involves the administration of appropriate blood schizonticidal drugs. In all cases of vivax malaria and in most cases of P. falciparum malaria, it involves the administration of chloroquine. In areas with high transmission of malaria, it is advisable to practice presumptive treatment for malaria.
Radical Treatment: Radical treatment is the administration of primaquine to all confirmed cases of malaria. In vivax malaria, 2 weeks' therapy with primaquine completely cure the infection in the host by its tissue schizonticidal activity and thereby prevents relapses. In P. falciparum malaria, a single dose of primaquine destroys the gametocytes, thereby prevents the spread of the infection into the mosquito 7, 8.
Mechanism of Action of Phytochemicals in Treatment of Malaria:
1. Amla:

FIG. 2: AMLA FRUITS
Synonym: Emblica, Indian goose berry, Amlaki.
Biological Source: It consists of dried, as well as fresh fruit of plant “Emblica officinalis”.
Chemical Constituents: Rich source of Vit-C, pectin, gallic acid, ellagic acid, IAA, glucose, and tannins. Vit-C indole acetic acid gallic acid ellagic acid pectin 12.
Activity of Drug: Promising anti-plasmodial activity was found in the extracts from E. officinalis leaf. They were also found to be active against chloroquine‑resistant strains.
These results demonstrate that extracts of E. officinalis may serve as anti-malarial agents even in their crude form. Pinmai et al., revealed that in-vivo anti-plasmodial activity with good suppression activity ranged from 53.40% to 69.46% 12, 13, 14, 15, 16, 17, 18.
2. Pomegranate:

FIG. 3: POMEGRANATE
Synonym: Pomegranate, Pom, anar.
Biological Source: It consists of oil obtained from dried seeds of “Punica granatum”.
Family: Puniacaceae.
Chemical Constituents: Pomegranate seeds yield a drying oil that contains Pucinic acid-forming upto 72% of the fatty acid.
Puccini acid is conjugated triene and a geometrical isomer of elaostearic acid, punicalin, and punicalagin.
Activity of Drug: Isolated gallagic acid and punicalagin exhibited anti-plasmodial activity against Plasmodium falciparum.
The daily intake of pomegranate juice as dietary supplements to augment the human immune system's anti-malarial and anti-microbial capacity.
3. Cinchona:

FIG. 4: CICHONA BARK
Synonym: Jesuit’s bark, Peruvian bark
Biological Source: “Cinchona calisaya, C. officinalis, C. succirubra”.
Family: Rubiaceae.
Chemical Constituents: Alkaloids (up to 15%) mainly quinoline alkaloids (quinine, quinidine), indole alkaloids (cinchonamine), bitter triterpene glycosides (quinovin), tannins, quinic acid.
Drug Activity: Cinchona alkaloids get concentrated in the acidic vacuoles of the blood schizonts and causes pigment changes, inhibits polymerization of heme to hemozoin. Free heme or heme-quinine complex damages parasite membrane & kill it.
4. Neem:

FIG. 5: NEEM LEAVES
Synonym: Margosa
Biological Source: It consists of fresh leaves extract of the plant “Azadirachta indica”.
Family: Meliaceae.
Chemical Constituents: Azadirachtin, meliantriol, salanin, nimbin, nimbidin, azadirachtin, kaem-pferol, myriciti deacetylaz adirachtinol, nimbin, nimbinin, nimbidin, margolone, margolone.
Activity of Drug: Neem has both curative and preventative effects on the malaria parasite; the methods for accomplishing this are as varied as the active ingredients in Neem. There are two compounds in Neem, which are clinically proven to be as effective against the malaria parasite as both quinine and chloroquine; they are gedunin, a limonoid, and quercetin, a flavonoid.
The leaves can be chewed and consumed on a daily basis as a preventative like quinine and neem leaf extracts are clinically proven to be as effective as chloroquine against the malaria parasite.
Neem leaf extracts prevent the normal development of the malarial plasmodia by increasing the state of oxidation in the red blood cells.
5. Artemisia:

FIG. 6: ARTEMISIA HERB
Synonym: Sweet-anne, Wormwood, quinghao.
Biological Source: It consists of traditional Chinese herb “Artemisia annua”.
Family: Asteraceae
Chemical Constituents: Artemisinin, artemether, artether, artemisinic acid.
Activity of Drug: Artemisinin shows antimalarial effects by its rapid blood schizonticidal activity. It is commonly used in tropical nations that can afford it, preferentially as part of a combination-cocktail with other anti-malarial in order to prevent the development of parasite resistance.
The end peroxide bridge in its molecule appears to interact with heme in the parasite. Iron mediated cleavage of the bridge releases a highly reactive free radical species that binds to membrane proteins, causes lipid peroxidation, damages endoplasmic reticulum, inhibits protein synthesis, and, ultimately, lysis of parasite. Artemisia is the most potent drug for treating cerebral malaria. Articulate and artemether have also been found to be highly effective.
6. Plumbago Benesis:

FIG. 7: FLOWERING TOPS OF PLUMBAGO BENESIS
Synonym: Plumago benesis
Biological Source: It consists of flowering tops of plant “Plumbago benesis”.
Family: Euphorbiaceae.
Chemical Constituents: Plumbagin, 3, 3’-plumbagin, 8, 8’-plumbagin.
Activity of Drug: Have in-vitro antimalarial activity against P. falciparum. Plumbagin Plumbago zeylenica and Cryptolepis sanguinolenta showed marked activity on the chloroquine-resistant and chloroquine-sensitive strains of Plasmodium falciparum. Plumbagin, a quinone, was isolated from Plumbago zeylenica and found to have antimalarial activity on chloroquine-sensitive and on chloroquine-resistant strains.
Cytotoxicity assays on KB cell lines indicated that the extract was selective for Plasmodium falciparum 12, 13, 14, 15, 16, 17.
7. Brucea javanica:

FIG. 8: BRUCEA JAVANICA
Synonym: Brucea javanica.
Biological Source: It consists of dried seeds of “Brucea javanica”.
Family: Simaroubaceae.
Chemical Constituents: Bruceoside A, Bruceoside B, Bruceine D, Bruceine E, Yadanzioside A, Yadanzioside G (20R)- O-(3)- α-L-arabino-pyranosyl- pregn-5- ene-3β, 20-diol and α-D-glucopyranoside.
Biological Activity of Drug: The leaf, root, and stem extracts of Brucea javanica were shown anti-malarial activity, after extractions with various organic solvents. Qualitative analysis of the phytochemical constituents showed the presence of the following secondary metabolites: terpenoids, saponins, flavonoids, steroids, phenols, glycosides, alkaloids and anthraquinones. The extracts showed very strong in-vitro activity against the malaria parasite Plasmodium falciparum. The phyto-chemical constituents in the extracts were also assessed. The acetone extract of the roots showed excellent anti-malarial activity, whereas stem and leaf extracts had high anti-malarial activities 12, 13, 14, 15, 16, 20.
8. Morinda lucida:

FIG. 9: STEM BARK MORINDA LUCIDA
Synonym: fruit, noni fruit.
Biological Source: It consists of dried leaves, stem bark, the root bark of “Morinda lucida”.
Family: Rubiaceae.
Chemical Constituents: Octoanoic acid, Scopoletin, Damnacanthal, Terpenoids, Anthra-quinones, Caproic acid, Ursolic acid, Rutin.
Activity of Drug: Morinda lucida extracts, the stem bark, the root bark, and the leaves show for anti-malarial activity against a chloroquine-sensitive strain of P. berghei in mice. Each extract produced a degree of suppression of parasitemia. The most promising result was obtained with chromatographic fractions of the stem bark extracts, the highest dose producing 96.4% suppression of parasite.
9. Cassia occidentalis:

FIG. 10: CASSIA OCCIDENTALIS
Synonym: Bamanan, Haussa. It is sometimes called coffee senna.
Family: Fabaceae.
Chemical Constituents: Alkaloids 0.13%, anthraquinones and a bianthraquinone, flavonoid glycosides matteucinol 7-rhamnoside and jaceidin 7-rhamnoside. Two new bis (tetrahydro) anthracene derivatives, occidentalol-1 Me and R2, and occidentalol-II were isolated from the roots of C. occidentalisalongue with chrysophanol, emodin, pinselin, questin, germichrysone, methyl-germitorosone and singueanol-I
Activity of Drug: The anti-malarial activity of C. occidentalis crude extracts was confirmed. The plant showed more than 60% inhibition of the parasite growth in-vitro. The ethanolic, dichloromethane and lyophilized aqueous extracts of Cassia occidentalis root bark was evaluated for their antimalarial activity in-vivo, suppressive assays against Plasmodium berghei in mice. All the ethanolic and dichloromethane extracts produced significant chemo suppressions of parasitaemia when administered orally 12-17.
10. Kalmegh:

FIG. 11: LEAVES OF KALMEGH
Synonym: Andrographis, Bhui-nimb
Biological Source: It consists of dried leaves and tender shoots of plant “Andrographis paniculata”.
Chemical Constituents: Kalmegh contain bitter principles and rographiolide, bicyclic diterpenoid lactones and kalmeghin.
Drug Activity: Methanolic extracts of the plant were tested in-vitro on chloroquine sensitive and resistant strains of Plasmodium falciparum for their anti-malarial activity. Growth inhibition was determined using different concentrations of these plant extracts on synchronized P. falciparum cultures at the ring stage. The performance herbal extract in isolation and combination was further evaluated in-vivo on mice infected with Plasmodium berghei 12, 13, 14, 15, 16, 17.
CONCLUSION: Nil
ACKNOWLEDGEMENT: Nil
CONFLICTS OF INTEREST: Nil
REFERENCES:
- WHO (1999), Roll Back Malaria: Increasing the momentum.
- WHO (1992), Entomological field technique for malaria control. Learner’s Russell Paul, West L. and Manwell R. (1946), Practical Malariology, WB Saunders Company.
- Planche T and Krishna S: The relevance of malaria pathophysiology to strategies of clinical management. Current Opinion in Infectious Dis 2005; 18(5): 369-75
- Andrej T, Matjaz J, Igor M and Rajesh M: Clinical review: Severe malaria. Critical Care 2003; 7: 315-23.
- Moody AH and Chiodini PL: Methods for the detection of blood parasites. Clin Lab Haematol 2000; 22: 189-01.
- Torres JR: Malaria and babesiosis. Therapy of Infectious Diseases Edited by: Baddour LM, Gorbach SL Philadelphia, PA: Saunders 2003; 597-13.
- Dondorp AM, Fanello CI and Hendriksen IC: "Artesunate versus quinine in the treatment of severe falciparum malaria in African children (AQUAMAT): an open-label, randomised trial". Lancet 376 (9753): 1647–57.
- Idro R, Otieno G, White S, Kahindi A, Fegan G, Ogutu B, Mithwani S, Maitland K, Neville BG and Newton CR: Malaria Journal 2005,4: 57.
- Jaypee Brothers: Essentials of Medical Pharmacology”, ed 5th - 2003, Medical publishers (P) Ltd., New Delhi 735-36.
- Kokate CK, Purohit AP and Gokhale SB: “Pharmacognosy”, edition 37th, Nirali Prakashan, 2007; 499-01, 369-70.
- Dwivedi S: “Medicinal Plants used to Cure Malaria”, Farmavita Net Journal 2007; 1-2.
- Mishra K, Dash AP, Swain BK and Dey N: “Antimalarial activities of Andrographis peniculata and H edyotis corymbosa extracts and their combination with curcumin”, Pubmed Central Journal 2009; 8: 1-10.
- Html., “Nation Institute of allergy and Infectious Diseases- Leading research to understand, treat and prevent infectious, immunologic and allergic diseases” 1-2; 35.
- Biswas, Kausik, Chattopadhyay I, Banerjee RK and Bandyopadhyay U: Biological activities and medicinal properties of Neem (Azadirachta indica). Current Science 2002; 82(11): 1336-45.
- Pinmai K: In-vitro and in-vivo antiplasmodial activity and cytotoxicity of water extracts of Phyllanthus emblica, Terminalia chebula and Terminalia bellerica. Journal of Medicinal Association Thailand 2010; 93: S12016.
- "A History of Mosquitoes in Massachusetts, by Curtis R. Best". Northeast Mosquito Control Association.
- Parinuch C and Theera S: Phytochemical and antimalarial screening of Brucea javanica plant extracts. Journal of Chem and Pharmaceutical Research 2014; 6(12): 253-56
How to cite this article:
Raut SS: Malaria and anti-malarial activity of medicinal plants: a review. Int J Pharmacognosy 2019; 6(12): 382-89. doi link: http://dx.doi.org/10.13040/IJPSR.0975-8232.IJP.6(12).382-89.
This Journal licensed under a Creative Commons Attribution-Non-commercial-Share Alike 3.0 Unported License.